Neural Considerations in Climbing Injuries – An Introduction
In this Rock Rehab Community lecture, sports musculoskeletal physiotherapist Julia Šmigelskis joins us live from Cape Town to break down the clinical application of neurodynamics for climbers and active athletes.
The session covers how peripheral nerve health influences movement quality, pain, and performance, with a practical focus on upper- and lower-extremity nerve mechanics commonly implicated in climbing-related complaints. Julia discusses when nerve symptoms are the primary driver versus a secondary contributor, how to interpret nerve sensitivity in assessment, and how to dose neurodynamic interventions without over-irritating the system.
This lecture is designed for clinicians, coaches, and serious climbers who want a clearer framework for integrating nerve-based assessment and treatment into rehabilitation and performance programming—moving beyond “stretching nerves” toward more precise clinical reasoning.
Topics Covered:
- Fundamentals of neurodynamics in sport and climbing
- Differentiating neural sensitivity from tissue and movement limitations
- Common nerve presentations in climbers
- Clinical reasoning for nerve-based interventions
- Practical progression and load management strategies
This is the first in a two-part series, with an advanced neurodynamics lecture planned later in the year.
Presenter Introduction
The content is presented by Julia Šmigelskis, a physiotherapist with academic training in both general physiotherapy and exercise and sports physiotherapy. Her background bridges clinical reasoning with performance-based rehabilitation, particularly relevant for climbers and active populations.

Shout Out
A brief acknowledgement of contributors, educators, and influences who have shaped the clinical approach and material presented in this talk.
Why Terminology Matters
Before discussing assessment and treatment, it’s important to clarify terminology. Neural pain is described using multiple overlapping terms in the literature, which can create confusion if definitions are not aligned. Understanding how these terms differ helps clinicians reason more accurately about pain mechanisms.

Neural Pain Terminology
This slide introduces commonly used terms such as peripheral neuropathic pain, nociceptive neural pain, and neurogenic inflammation. Multiple different terms are used to describe neural disfunction in the literature. For the purpose of this discussion the ANMS based terminology peripheral neurogenic pain and nociceptive neural pain will be used.
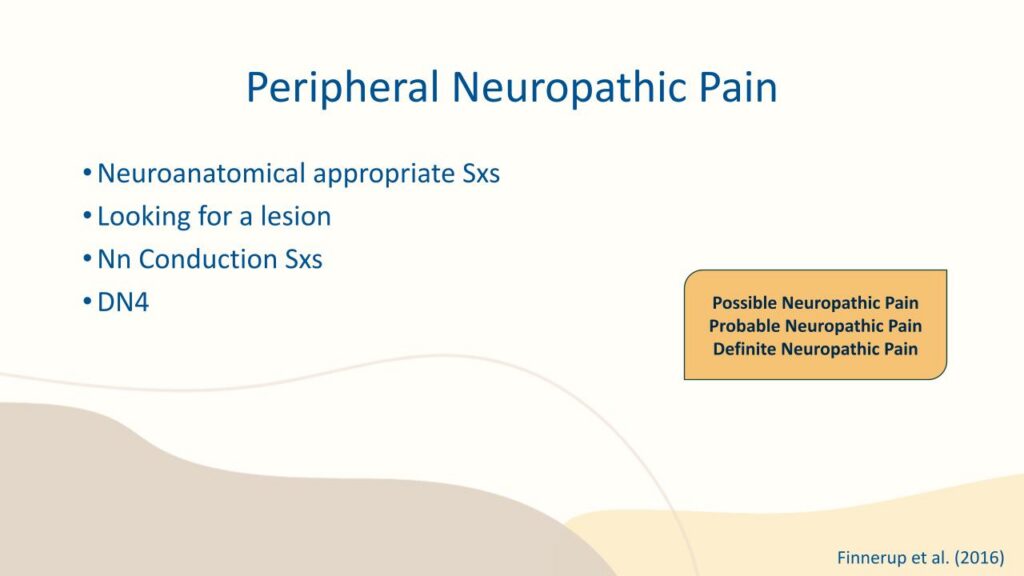
Peripheral Neuropathic Pain
Peripheral neuropathic pain is characterised by symptoms that follow a neuroanatomically logical pattern. Clinically, this often involves identifying a lesion or injury to the nerve itself, along with conduction-related symptoms such as sensory loss, altered reflexes, or weakness. Tools like the DN-4 assist in classifying possible neuropathic pain as probable neuropathic pain. Yet, for a confirmed definitive neuropathic pain diagnosis, positive imaging must be present.
Nociceptive Neural Pain
Nociceptive neural pain refers to sensitisation of peripheral nerves without a clear structural lesion. Pain arises from the nervi nervorum—the small nerves supplying the nerve sheath itself—and is often driven by compression or tension that compromises blood supply. This concept reinforces the idea that nerves are highly sensitive to mechanical and vascular stress.

Introduction to Neural Anatomy
A foundational understanding of neural anatomy is essential when assessing nerve-related pain. Visualising how nerves move, adapt, and interact with surrounding tissues provides context for both symptom presentation and treatment strategies.
Visual Anatomy Reference
This slide uses 3D anatomical visuals to illustrate nerve pathways and their relationship to surrounding structures, reinforcing the importance of spatial awareness in clinical reasoning.
For ease of visualisation in the climbing population, the nervous system of the arms and legs can be compared to a sport climbing rope system.
The nerve can be seen as the “rope” that travels up one side, passes through the vertebra (functioning as the “chains”), and then descends down the other side. The muscles and connective tissue that the nerves travel through act as the “quick draws.”
When chains become “stiff” or quick draws become “tight,” rope drag increases. In the same way, restrictions in joints, muscles or connective tissue increase mechanical stress on the nervous system.
C2 is a crucial link in this chain, as the dura mater extends down to this vertebra. A systematic review by Palomeque-Del-Cerro et al. (2017) highlighted that multiple short extensor muscles have connective tissue connections to the dura. Therefore, the upper cervical area — often placed under sustained stress during belaying or prolonged upward gaze while climbing — may play a role in altered or limited neural dynamics.
Nervous System Assessment Overview
Effective assessment begins with considering the nervous system as a potential driver of symptoms. This requires intentional questioning and structured examination, rather than assuming pain is purely muscular or joint-based.

The Interview: Listening for Neural Clues
Patient history is critical. Clinicians should pay close attention to how symptoms are described, what aggravates or eases them, and whether symptom patterns suggest neural involvement. Often, the interview provides the strongest clues before physical testing begins.
Neural pathways across joints and movement chains
Anatomical visualisation showing how peripheral nerves traverse multiple joints and regions, reinforcing the concept that neural symptoms may be influenced by movement or position away from the site of pain. Highlights in blue show common nerve-related areas of complaint.
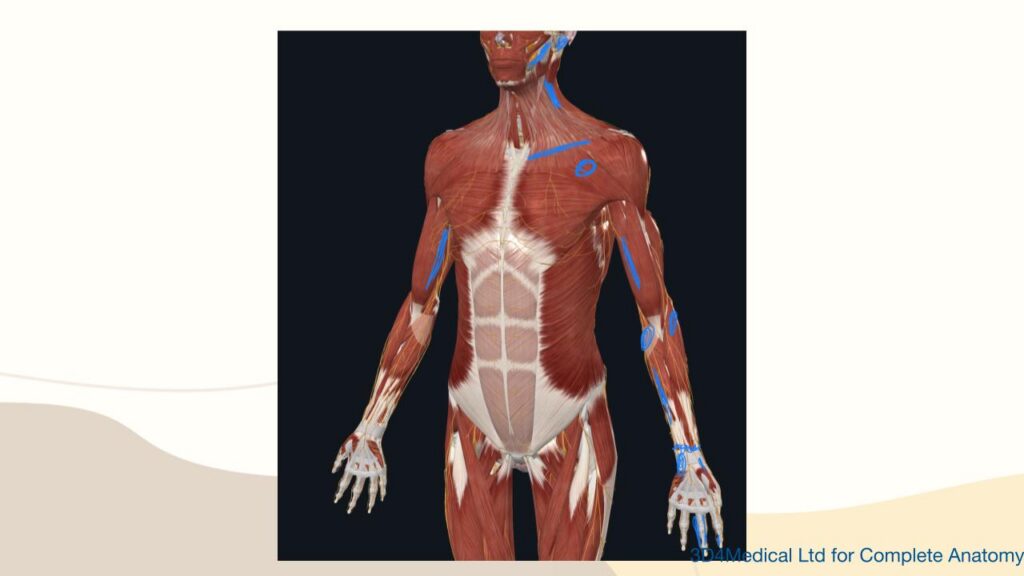
Peripheral nerves and muscular interfaces
Anterior view illustrating peripheral nerves in relation to major muscle groups of the upper body. This highlights common interfaces where neural structures may be exposed to compression or increased tension during climbing-specific postures and loading.

Mechanism of Injury and Symptom Onset
Understanding how symptoms started helps differentiate between traction-based and compression-based neural mechanisms. Timing, load exposure, and progression of symptoms all inform clinical reasoning.
Climbing-Specific Traction Mechanisms
In climbers, traction-related neural stress can occur during activities such as carrying heavy bouldering pads, prolonged belaying with extended cervical extension, dry firing, uncontrolled dynos, or sudden foot pops that place unexpected load through the upper limb.
Climbing-Specific Compression Mechanisms
Compression-related neural irritation often results from increased muscle tone, shortened tissues, postural habits, or excessive scapular setting. These factors can reduce available space for neural structures, particularly during repetitive or sustained climbing positions.
Physical Evaluation Overview
Physical assessment should include active range of motion of the cervical, thoracic, and lumbar spine, with consideration of whether symptoms are driven more by compression or traction. Both neural conduction testing and neurodynamic assessment play a role, alongside palpation and special tests.

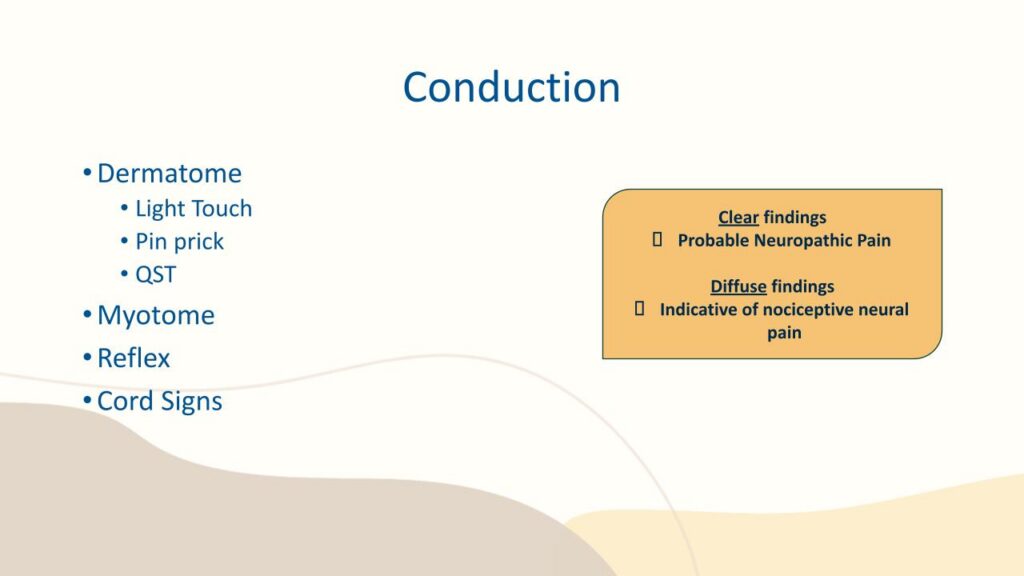
Neural Conduction Testing
Conduction testing examines dermatomes, light touch, pinprick sensation, myotomes, reflexes, and potential spinal cord signs. Clear, localised findings tend to indicate probable neuropathic pain, while diffuse or inconsistent findings are more suggestive of nociceptive neural pain.
Neurodynamics in Assessment
Neurodynamic testing helps differentiate whether neural structures contribute to symptoms during movement. Tests such as upper limb tension tests, slump, and straight leg raise assess the nervous system’s mechanical sensitivity and adaptability.
Interpreting Neurodynamic Tests
The quality of test execution and interpretation is critical. Neurodynamic tests are not simply about reproducing pain, but about understanding how symptom behaviour changes with structural differentiation and movement elsewhere in the system.
Common Findings in Climbers
Climbers frequently present with a depressed or anteriorly rotated shoulder girdle, increased tone or shortening in muscles such as pectoralis minor, biceps, brachialis, brachioradialis, and forearm flexors. Other common findings include lumbrical shift syndrome, hip flexor tension from steep climbing, and heel hook–related injuries.
Introduction to Treatment
Treatment of neural pain requires careful load management and ongoing reassessment. Interventions must be matched to the severity, intensity, and nature of symptoms rather than applying a one-size-fits-all approach.

Treatment Principles
Treatment intensity should align with SIN findings. Key strategies include interface release, neural mobilisation (progressing from gliders to tensioners), and gradual return to climbing. Neural conduction should be continually reassessed to guide progression.
High SIN and Acute Presentations
In cases of very high severity or acute symptoms, immediate referral may be required. Early management focuses on offloading, taping, rest, ice, and following the POLICE protocol to protect neural tissue.
General Interface Release
General techniques aim to improve space and movement around neural structures. These may include spinal mobilisations, first rib techniques, gentle soft tissue work, and fascial approaches such as skin rolling.
Specific Neural Mobilisation Techniques
More targeted mobilisation techniques address specific interfaces, such as cervical transverse glides, lumbar opening techniques, glenohumeral and radial head mobilisations, forearm rotational work, carpal mobilisations, and proximal tibiofibular techniques.

Identifying the Primary Interface
A key clinical question is identifying which muscular or structural interface is most responsible for neural irritation, guiding more precise intervention.

Gliders vs Tensioners
This slide invites reflection on when to use neural gliding techniques versus tensioning techniques, emphasising clinical reasoning rather than rigid protocols.
Returning to the climbing rope analogy, one can visualise that a rope thins under stretch. The same applies to nerves, where the result is a reduction in blood supply. A sensitised nervous system responds with symptoms, pain and increased muscle tone to reduced circulation. Therefore, gliders should be chosen over tensioners in the acute or neurally sensitised patient until the system is ready to be challenged by re-introducing tension.
Returning to Climbing
Return-to-climbing strategies should include specific warm-ups, reducing foot pop risk, adjusting wall angle, controlled movement within a small climbing box, and careful dosage. Clinicians must watch for latent symptom responses and early warning signs.
Stretching Considerations
Stretching is addressed cautiously, recognising that aggressive stretching may aggravate neural symptoms rather than resolve them, depending on the underlying mechanism.

Questions
An opportunity for discussion, clarification, and application of concepts to real-world climbing scenarios.
References
The presentation concludes with key references supporting the concepts discussed, including work on neuropathic pain classification and anatomical connections between neural and musculoskeletal structures.
- Disclaimer – The content here is designed for information & education purposes only and the content is not intended for medical advice.

Related Posts