Thoracic Outlet Syndrome (TOS) in Climbers
In this Rock Rehab Community lecture, physical therapist and climber Dr. TH David joins us to break down the clinical assessment and rehabilitation of thoracic outlet syndrome in rock climbers — a condition he has titled How to Catch a Ghost.
The session covers the three types of TOS, relevant anatomy, and how to identify neurogenic presentations in the clinic. TH draws on his own experience as both a clinician and someone who lived with undiagnosed TOS for years, sharing practical insights around latissimus involvement, scapular positioning, force vectors, and climbing-specific movement analysis.
This lecture is designed for medical providers who want a clearer clinical framework for identifying and treating this notoriously elusive diagnosis in their climbing patients.
Topics Covered:
- Types of thoracic outlet syndrome and relevant anatomy
- Clinical presentations and examination findings in neurogenic TOS
- Current evidence for conservative TOS treatment
- Latissimus involvement and scapular positioning as a clinical hypothesis
- Biomechanics, force vectors, and climbing movement analysis
- Exercise progressions and climbing-specific drills for return to climbing
How to Catch a Ghost
Thoracic outlet syndrome (TOS) has a reputation for being one of the most difficult diagnoses to pin down in clinical practice — elusive, variable, and easily mistaken for something else entirely. In this Rock Rehab Community lecture, TH David walks through his approach to identifying and treating neurogenic TOS in rock climbers, drawing from clinical experience, research, and his own history with the condition.
Introduction
TH’s path to physical therapy was unconventional. Before PT school, he spent four years as a production potter — work that gave him firsthand experience with repetitive strain. He completed his BA in Studio Art at St. Olaf College and his DPT at CU Anschutz in 2020.
He has been climbing since 2012 and now runs Mend & Send PT and Performance, a climbing-focused cash practice based inside Big Island Bouldering. He also works one day per week at Motion St. Paul treating elbow, wrist, and hand conditions alongside climbers.
My TOS Journey
TH’s interest in this condition is personal. For roughly five years he experienced deep, bilateral aching pain radiating down both triceps — worsening with activity and most noticeable after releasing from the climbing wall rather than during loading. He was diagnosed with tricep tendinopathy, rehab made no difference, and direct tricep loading produced no symptoms at all. It was only in PT school that the picture became clear — he tested positive for every TOS special test, with full symptom recreation during the supraclavicular compression test. He has now been symptom-free for six years.
Objectives
TH outlines the major goals of the presentation. The talk is designed to help clinicians better understand thoracic outlet syndrome, improve diagnostic reasoning, appreciate the complexity of the condition in climbers, and explore rehabilitation strategies that can be adapted to individual movement patterns.

Why Does This Matter?
TOS affects between 3 and 80 people per 100,000 in the general population, with overhead athletes at higher risk. It is a diagnosis of exclusion, easily misdiagnosed, and can be chronic and disabling for months to years. If caught, up to 95% of patients can achieve full resolution — though that figure is limited by how difficult the condition is to track. Clinically, many of TH’s patients with TOS had been previously misdiagnosed and had failed prior physical therapy before finding their way to an accurate diagnosis.

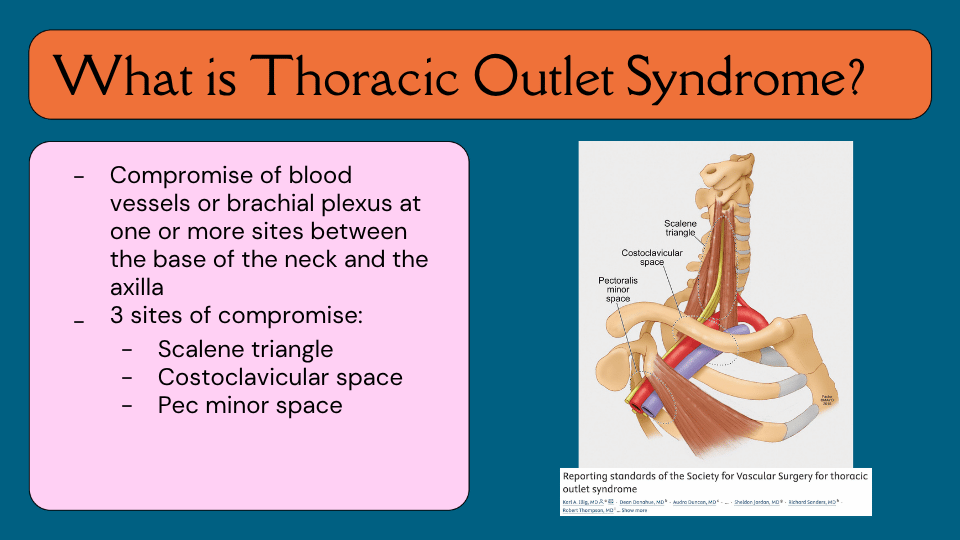
What Is Thoracic Outlet Syndrome?
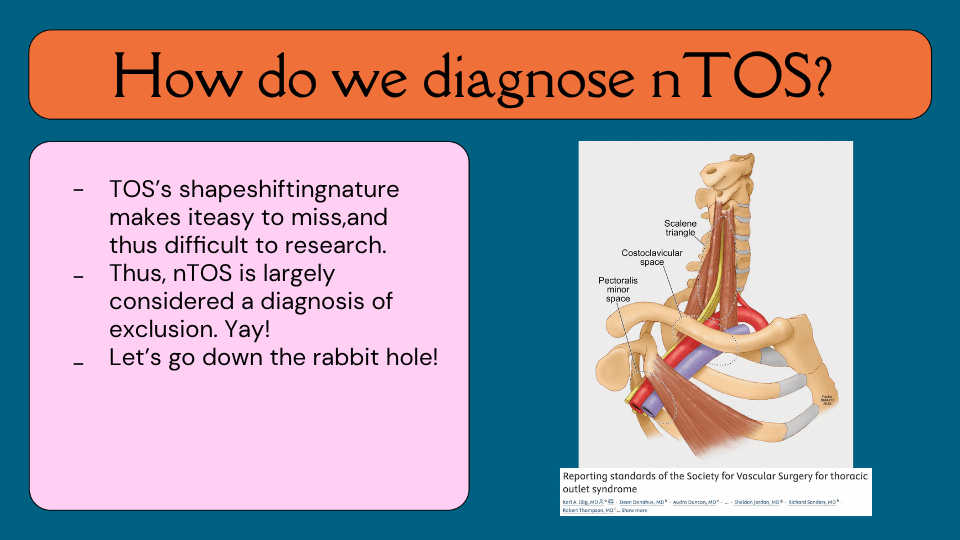
At its broadest, thoracic outlet syndrome refers to compromise of the blood vessels or brachial plexus at one or more sites between the base of the neck and the axilla. There are three primary sites where this compromise can occur: the scalene triangle, where the brachial plexus passes between the anterior and middle scalene muscles; the costoclavicular space, the corridor between the clavicle and the first and second ribs; and the pectoralis minor space, where the neurovascular bundle continues beneath the pec minor before reaching the axilla. Think of it as a three-part tunnel, and the structures travelling through it can be compressed at any one — or more — of these points.
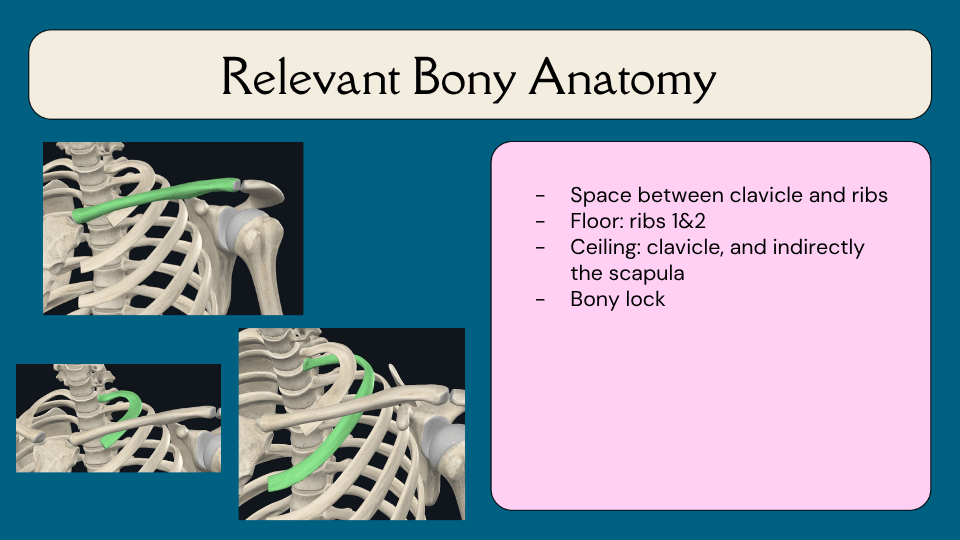
Relevant Bony Anatomy
The costoclavicular space is defined by a floor and a ceiling. The floor is formed by the first and second ribs. The ceiling is the clavicle — and indirectly, the scapula. Because the clavicle is the only bony connection the scapula has to the rest of the skeleton, wherever the scapula goes, the clavicle follows. This means scapular position has a direct influence on the size of the space available for the neurovascular bundle. When the clavicle and scapula descend toward the ribs, that space narrows — a concept TH returns to repeatedly throughout the presentation when discussing scapular depression and its potential role in TOS.
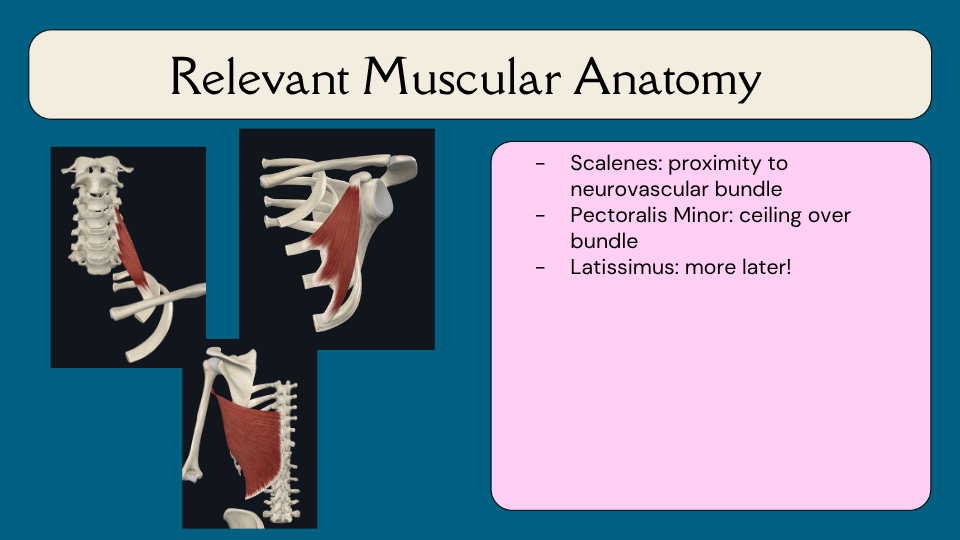
Relevant Muscular Anatomy
The muscles most commonly discussed in relation to TOS are the scalenes, which sit in close proximity to the neurovascular bundle as it exits the scalene triangle, and the pectoralis minor, which forms the ceiling over the bundle as it passes through the subcoracoid space. TH also flags the latissimus dorsi here — with a note that more on its potential role will come later in the presentation.
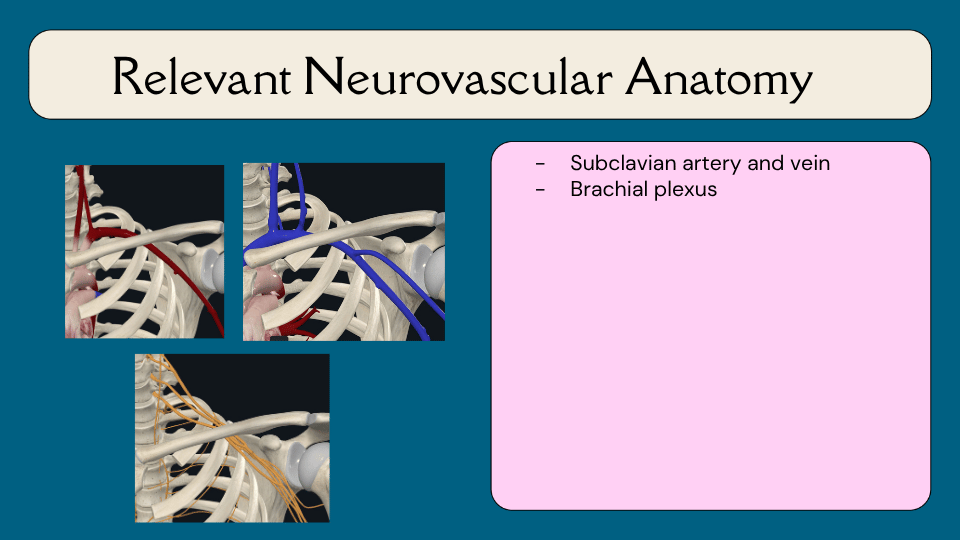
Relevant Neurovascular Anatomy
Three structures are at risk of compromise as they travel through the thoracic outlet: the subclavian artery, the subclavian vein, and the brachial plexus. Because different structures can be affected, thoracic outlet syndrome can present in quite different ways depending on which of these is being compressed — which is why the three types of TOS vary so significantly in their clinical picture.
Types of TOS
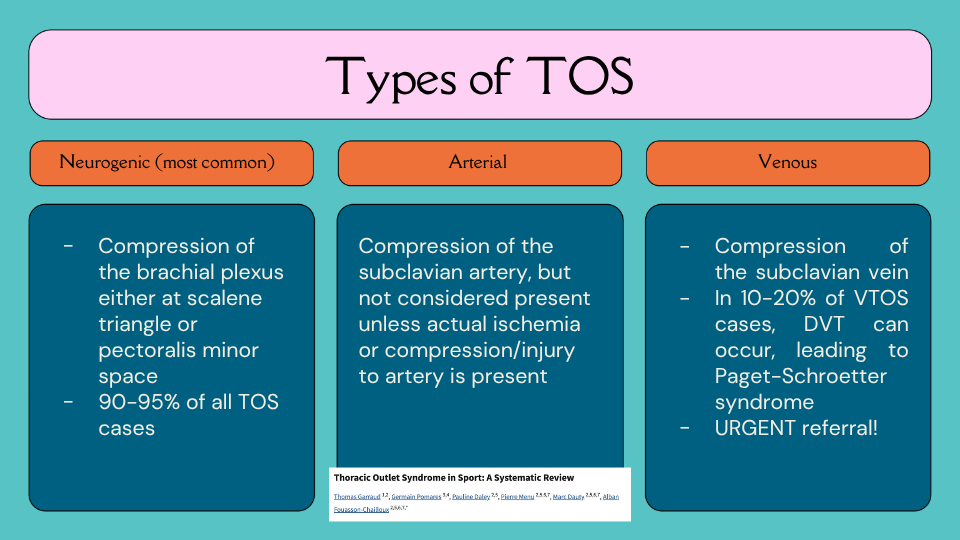
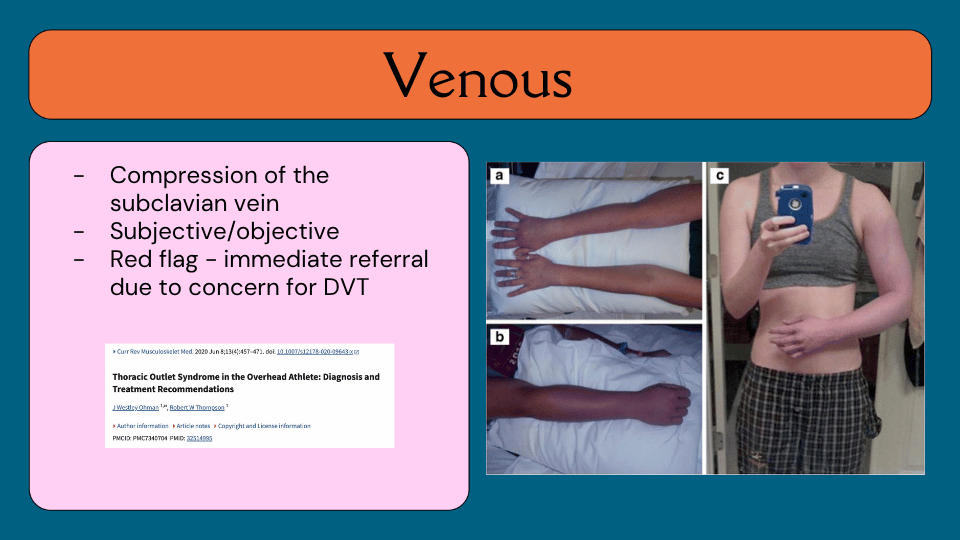
There are three types of thoracic outlet syndrome, each defined by the structure being compressed. Neurogenic TOS involves compression of the brachial plexus and accounts for 90–95% of all TOS cases — it is the primary focus of this presentation. Arterial TOS involves compression of the subclavian artery, but is only considered present when actual ischemia or injury to the artery is confirmed on examination. Venous TOS involves compression of the subclavian vein, and in 10–20% of venous TOS cases, a DVT can develop, leading to Paget-Schroetter syndrome — an urgent referral that TH notes he has fortunately never encountered in clinic, but describes as unmistakable when present.
Neurogenic TOS
Neurogenic TOS is compression of the brachial plexus, thought to occur either at the scalene triangle or the subcoracoid space. As the most common form by a wide margin, it is what clinicians are most likely to encounter — and what the remainder of this presentation addresses in detail.

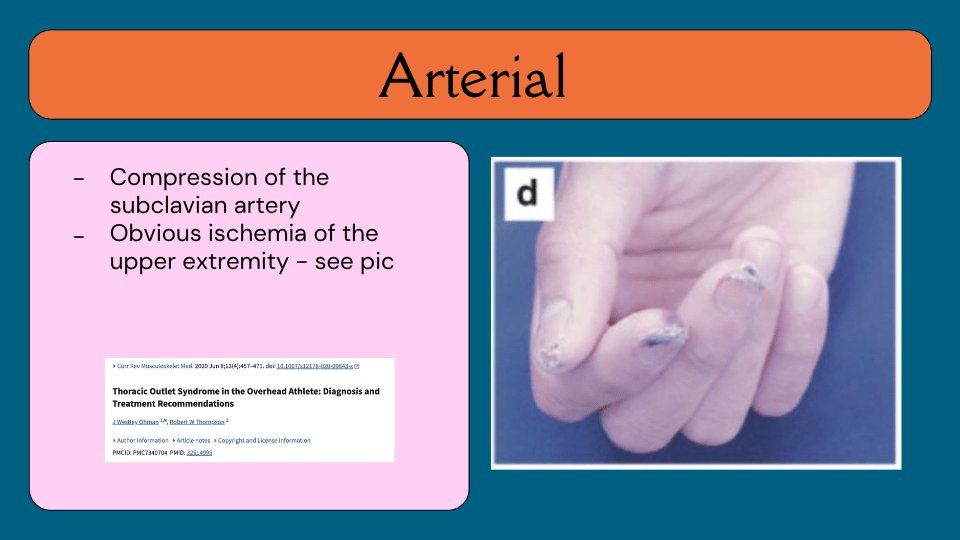
Arterial TOS
Arterial TOS involves compression of the subclavian artery severe enough to cause obvious ischemia of the upper extremity. Clinically this can present as skin breakdown or discoloration at the fingertips due to lack of blood flow — a presentation that is visually distinct and not easily confused with neurogenic TOS.
Venous TOS
Venous TOS involves compression of the subclavian vein and is an immediate red flag. A visibly swollen, discolored arm — particularly with color changes that are asymmetric and position-independent — warrants urgent referral due to the risk of deep vein thrombosis. TH describes this as a presentation that, if you see it, you will know.
Overhead Athletes and TOS
Overhead athletes carry a slightly elevated risk of developing TOS, though the data here is limited. What TH observes clinically — without yet finding literature to support it — is that TOS frequently presents alongside hypermobility, specifically in patients scoring above 4 out of 9 on the Beighton scale. He flags this as an area he would love to see studied, and offers potential hypotheses for the connection later in the presentation.
How Do We Diagnose Neurogenic TOS?
This is where things get honest. TOS is notoriously difficult to research precisely because it is so difficult to diagnose — its shapeshifting nature means it is easy to miss, easy to misattribute, and hard to track in the literature. As a result, neurogenic TOS is largely considered a diagnosis of exclusion. There is no clean algorithm. TH’s invitation to the audience at this point is simply: let’s go down the rabbit hole together.
Neurogenic TOS: Clinical Presentation Overview
The clinical picture of neurogenic TOS has three broad components. Subjectively, there is enormous variability — but there are certain patterns worth listening for. Objectively, very few findings are actually diagnostic, though they can help build a clinical picture. And special tests, as TH puts it, are kind of a nightmare — they have their place, but the research does not hold your hand.
Patient-Reported Outcome Measures
For tracking patient progress, TH primarily uses the QuickDASH, which has the strongest recommendation in the literature and good correlation with perceived disability. Two additional measures mentioned in the research are the Cervical-Brachial Symptom Questionnaire and the SF-12 for assessing quality of life. TH notes these are what the research supports, though he also uses climbing-specific outcome measures in his own practice.
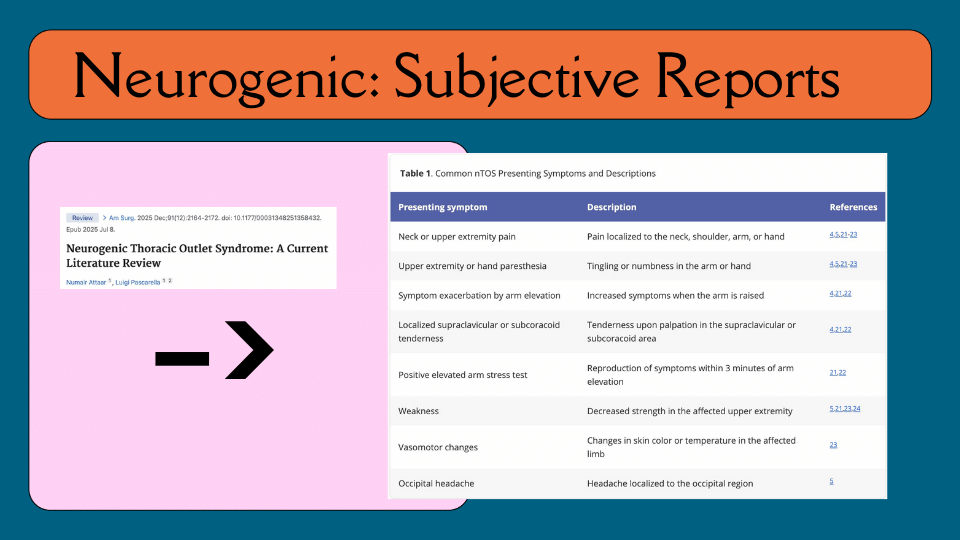
Neurogenic TOS: Subjective Reports
The list of common neurogenic TOS symptoms is broad enough to overlap with almost any upper extremity condition — which is precisely what makes this diagnosis so easy to miss. Common presentations include pain localized to the neck, shoulder, arm, or hand; tingling or numbness in the arm or hand; increased symptoms when the arm is raised; localized supraclavicular or subcoracoid tenderness; a positive elevated arm stress test; weakness or decreased strength in the affected upper extremity; vasomotor changes such as altered skin color or temperature; and occipital headache. The challenge is that individually, any one of these could point to a dozen other diagnoses.
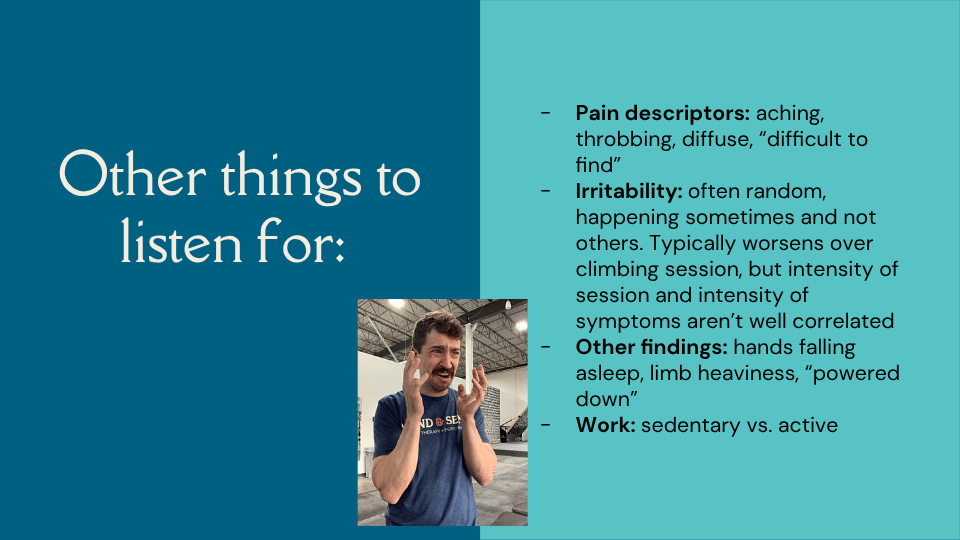
Other Things to Listen For
Beyond the standard symptom list, TH has identified several patterns in his climbing patients that raise his index of suspicion for TOS. Pain descriptors tend to be aching, throbbing, or diffuse — the kind of pain the patient cannot locate by pressing on anything. Irritability is often random, happening on some sessions and not others, typically worsening over the course of a climbing session but without a clear relationship between session intensity and symptom intensity. Other common reports include hands falling asleep more regularly than usual, a sense of limb heaviness, or feeling suddenly “powered down” during a session. TH also notes the value of asking about work — whether the patient is sedentary at a desk all day or physically active — as this shapes the approach to treatment.
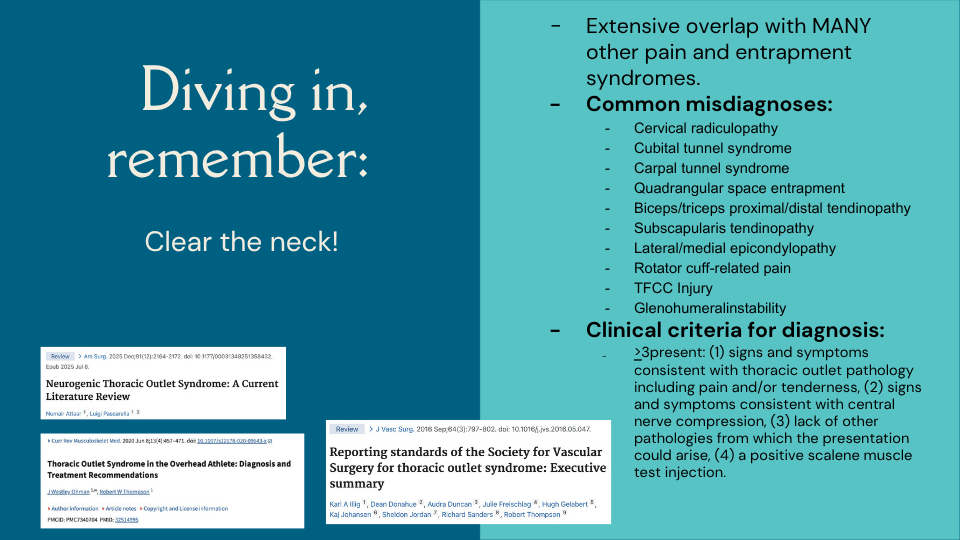
Diving In: Clear the Neck
Before pursuing a TOS diagnosis, clearing the cervical spine is essential — the overlap with other conditions is extensive. Common misdiagnoses include cervical radiculopathy, cubital tunnel syndrome, carpal tunnel syndrome, quadrangular space entrapment, biceps and triceps tendinopathy, subscapularis tendinopathy, lateral and medial epicondylopathy, rotator cuff-related pain, TFCC injury, and glenohumeral instability. The clinical criteria for diagnosis require three or more of the following to be present: signs and symptoms consistent with thoracic outlet pathology including pain or tenderness; signs and symptoms consistent with central nerve compression; lack of other pathologies that better explain the presentation; and a positive scalene muscle injection test. For physical therapists working in conservative management, the first three criteria are what matter most.
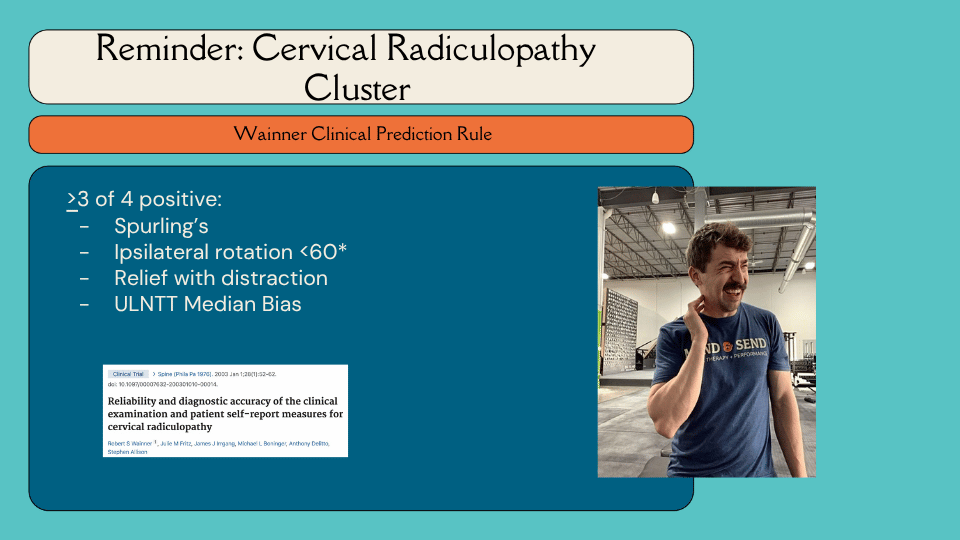
Reminder: Cervical Radiculopathy Cluster
Because neurogenic TOS can look so much like cervical radiculopathy, TH includes a reminder of the Wainner Clinical Prediction Rule. Three or more of the following four findings suggest cervical radiculopathy: a positive Spurling’s test; ipsilateral rotation of less than 60 degrees; relief with cervical distraction; and a positive upper limb neural tension test with a median nerve bias. TH has seen many patients arrive with a cervical radiculopathy diagnosis who were negative for all four of these findings — a pattern that redirected his clinical suspicion toward TOS.
Objective Findings
On the objective side, the findings that have actually been correlated with TOS in the literature are hand dynamometry and internal and external rotation strength testing. Beyond those, TH also assesses scaption, rhomboids, middle and lower trapezius strength, and range of motion measures including pectoralis minor length, pectoralis major length, and latissimus length. He notes that for his hypermobile patients, length testing is often unrevealing. Posture and scapular mechanics round out the assessment — not because the research supports a direct link to pain, but because they contribute to the overall clinical picture.

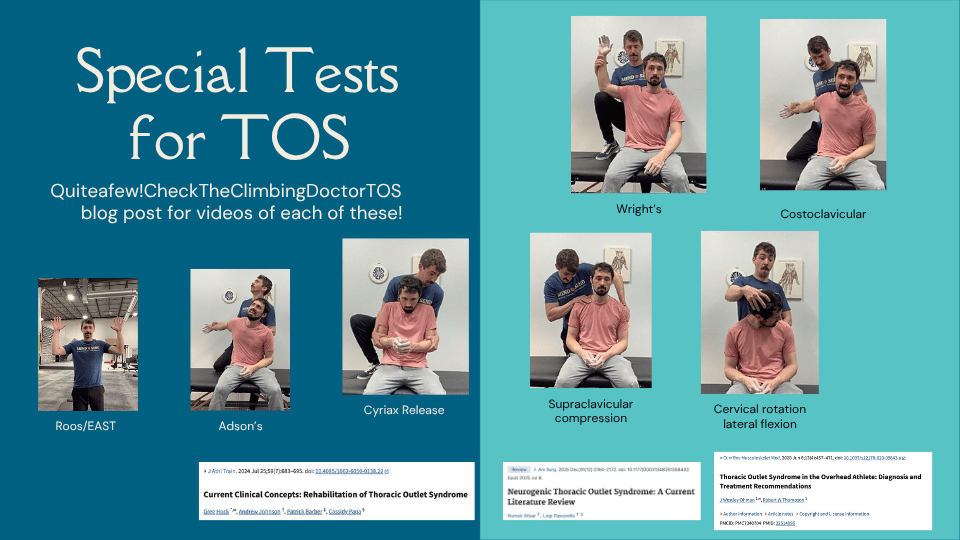
Special Tests for TOS
There are six special tests commonly used for TOS: the Roos/EAST test, Wright’s test, the Costoclavicular test, Adson’s test, the Supraclavicular Compression test, the Cervical Rotation Lateral Flexion test, and the Cyriax Release test. TH notes that Jared has an existing blog post on The Climbing Doctor website with videos demonstrating each of these tests — a useful reference for anyone wanting to review technique. He also notes that taking the photos for this slide with his colleague got progressively sillier as they went, which the images confirm.

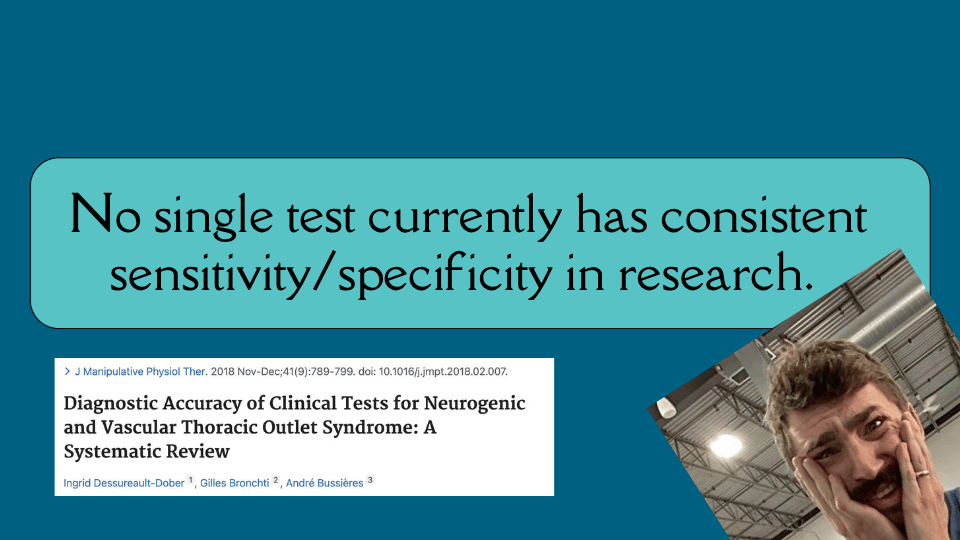
No Single Test Has Consistent Psychometrics
Here is the uncomfortable truth: not a single special test for TOS currently has consistent sensitivity or specificity in the research. Not one. They can contribute to a clinical picture, but none can reliably rule TOS in or out on its own. This is a significant limitation, and TH is candid about it.

TOS Is About Questions, Not Answers
Stepping back from the diagnostic detail, TH frames the big picture honestly. If TOS is a diagnosis of exclusion, what happens when it co-exists with another condition? How important is a precise diagnosis when the diagnosis itself is so vague? If no objective findings strongly correlate with TOS, how do we track whether treatment is working? And even with poor psychometrics, might the positional demands of the special tests still have value given how closely they mirror climbing positions? These are the questions TH sits with — and invites the audience to sit with too.
Personally
TH’s personal approach is to treat TOS as something he is varying degrees of suspicious of, rather than something he definitively rules in or out. In climbing, he is particularly suspicious that TOS may arise from specific strategies climbers use when pulling on holds. He also brings patients into his thinking — being transparent that the picture is messy, but that it is possible to make progress.
PT vs Surgery
Conservative management outcomes for neurogenic TOS range widely — from 39% to 95% depending on the study. Non-surgical options include Botox injections to the scalenes or pectoralis minor, which have shown some promising results. Surgical options include first rib resection, scalenectomy, and pectoralis minor release — procedures that, as TH notes, sound far more routine than they actually are. He is personally attached to his first rib, and finds that most of his patients feel the same way.
PT Philosophy and Approach
A systematic review by Luu et al. examined exercise interventions for neurogenic TOS and found something striking: even approaches with conflicting philosophies — one group depressing the scapula, another elevating it — both produced positive outcomes. Every group got better. The range of approaches studied includes posture correction, breathing training, scapular elevation and depression, scapular mechanics, nerve glides, general strengthening, joint mobilizations, manipulation, and dry needling. Of all of these, the only intervention with solid Level A evidence is exercise. Everything else sits at Level B or C. The authors’ key recommendation is a biopsychosocial approach — because exercise works, and the philosophy matters less than you might think.
Big Takeaway: Exercise Works
The practical implication of this is significant. If you are suspicious that a patient has neurogenic TOS and you do exercise with them, they will probably get better — regardless of the specific approach. The worst outcome is not catching it at all. And if you are already treating the shoulder and surrounding musculature, as TH does with most of his climbing patients regardless of diagnosis, symptoms are likely to improve anyway. This also means there is a lot of room for curiosity and experimentation — which TH finds considerably more appealing than a rigid diagnostic-treatment algorithm.
The Land Ahead Is Muddy
From this point forward, TH is clear that what he is sharing is based on his own clinical questions, biomechanical reasoning, movement observations, and personal experience — not established research. The content ahead may not align with how others approach TOS, and that is entirely fine. He may revisit these slides in five years and land somewhere different. For now, this is what is exciting him clinically.

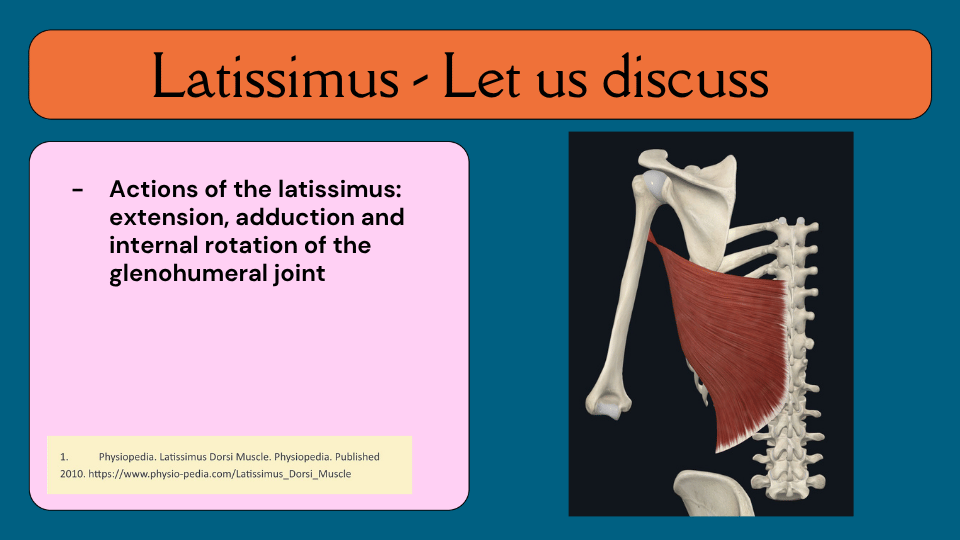
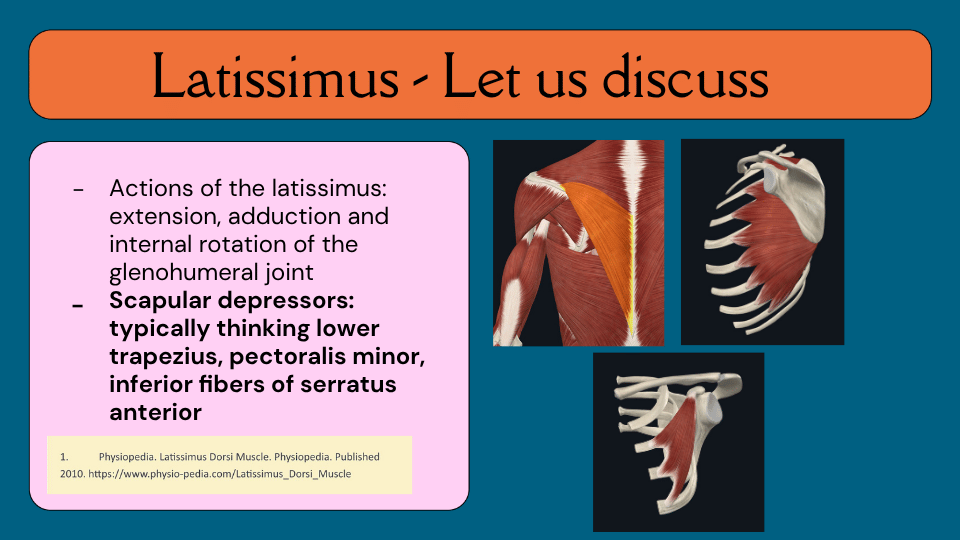
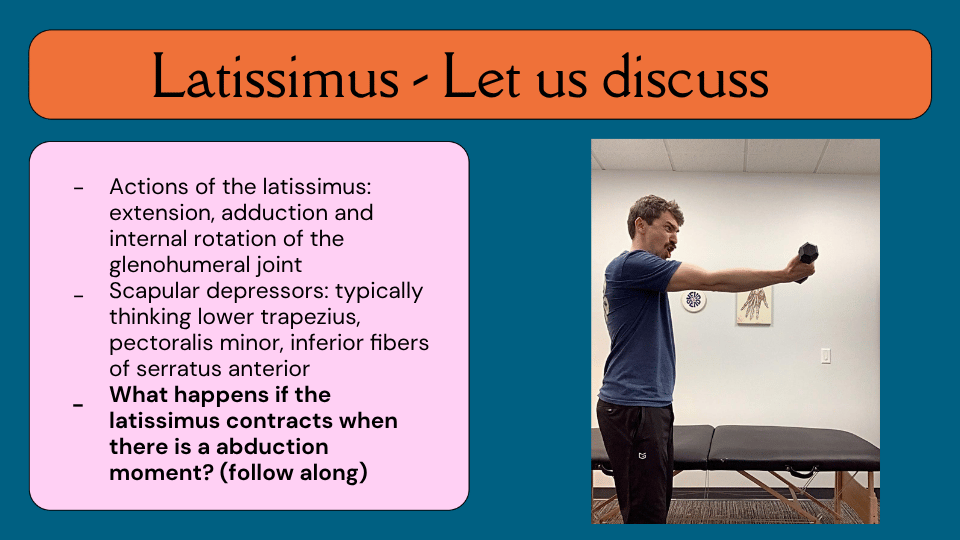
Latissimus: Let Us Discuss
The latissimus dorsi is classically described as performing glenohumeral extension, adduction, and internal rotation. The muscles typically identified as scapular depressors are the lower trapezius, pectoralis minor, and inferior fibers of the serratus anterior. But TH poses a question: what happens when the latissimus contracts during an abduction moment? He invites the audience to follow along — hold the arm out to the side in scaption, palpate the latissimus, and then actively depress the scapula. For many people, the latissimus engages — despite no adduction, extension, or internal rotation being performed. TH’s hypothesis is that in this context, the latissimus may be acting as a scapular depressor rather than a glenohumeral mover.
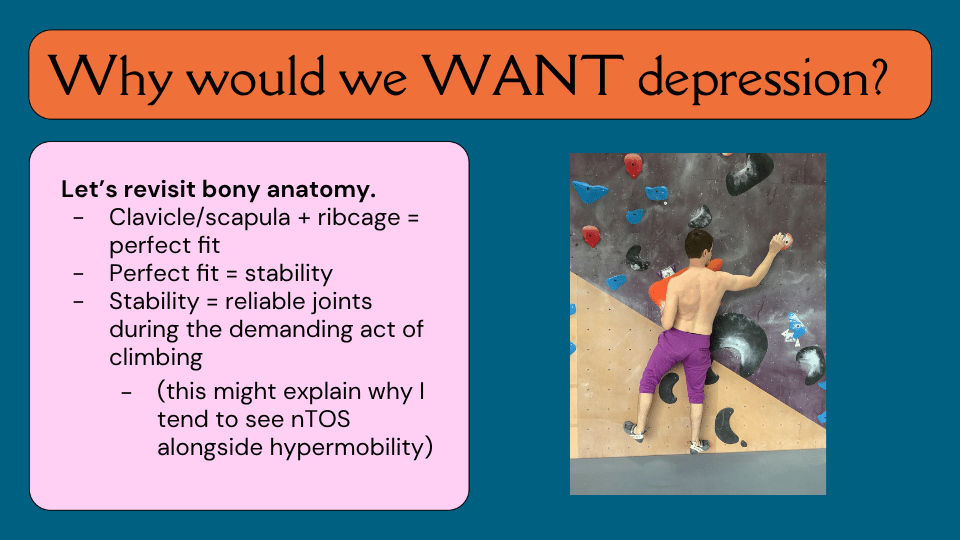
Why Would We Want Scapular Depression?
The clavicle, scapula, and rib cage form a near-perfect bony fit. Locking that system down through depression creates a highly stable joint — reliable and predictable during the demanding, closed-chain movements of climbing. For hypermobile climbers in particular, who may have difficulty generating passive stability through their joints, this strategy may feel essential. TH suspects this is why he tends to see neurogenic TOS more frequently in patients who score higher on the Beighton scale — though he acknowledges no research currently supports this observation.
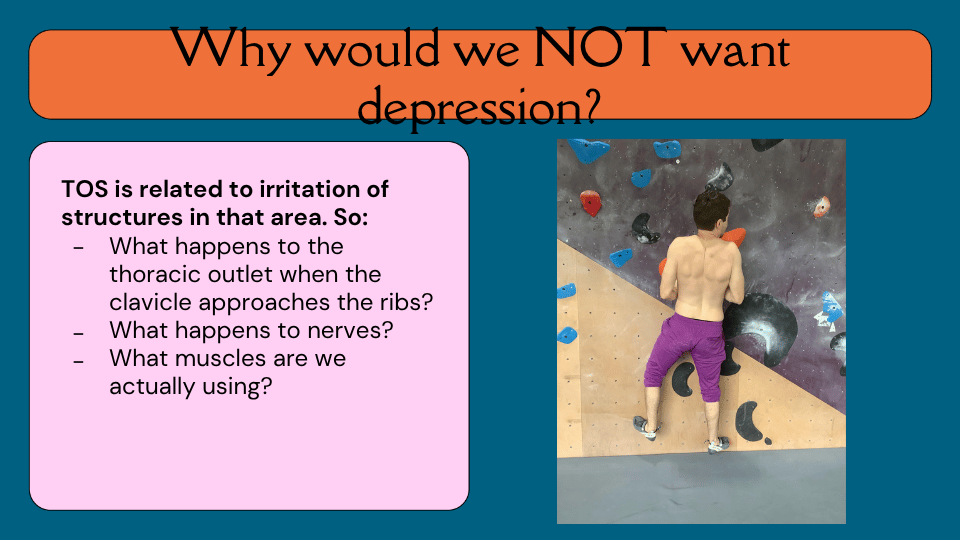
Why Would We NOT Want Scapular Depression?
The problem is the trade-off. When the clavicle approaches the ribs — which is exactly what happens during scapular depression — the space through which the brachial plexus travels narrows. Nerves get compressed. And if the latissimus is contributing to that depression, the muscles involved may be different from what we typically assume. TH is careful to note that the research clearly shows the philosophy of treatment does not matter — so this is not a definitive claim, but a clinical question worth exploring.

Therefore: “Down and Back” Might Not Always Be the Answer
The classic postural cue of scapular depression and retraction — down and back — is one of the most common instructions given in shoulder rehabilitation. TH argues that in the context of neurogenic TOS, particularly for climbers who may already be relying heavily on depression as a stability strategy, this cue may be counterproductive. He proposes that a gentle shrug during load might actually have benefits worth exploring.


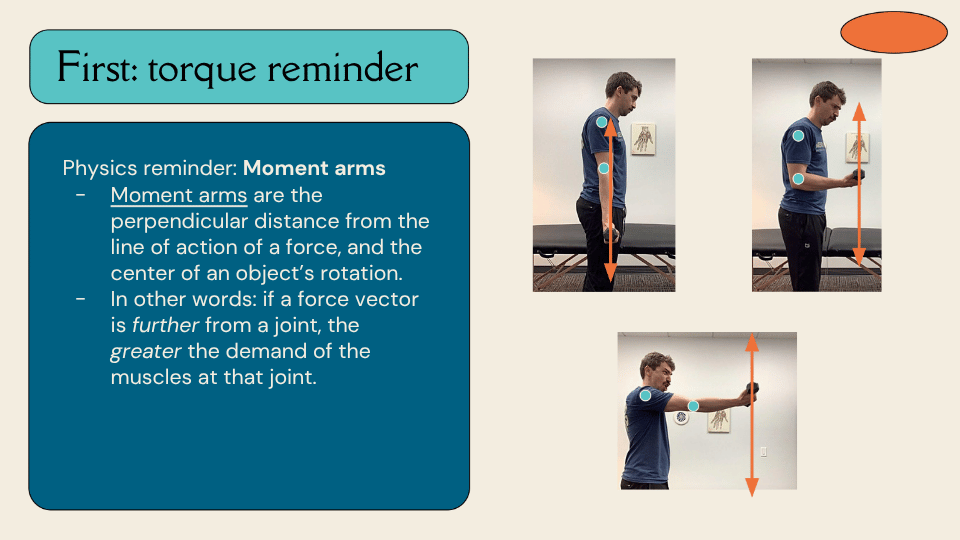
First: A Torque Reminder
To understand why scapular position matters biomechanically, TH offers a reminder about moment arms. A moment arm is the perpendicular distance from the line of action of a force to the centre of an object’s rotation. In practical terms: the further a force vector is from a joint, the greater the muscular demand at that joint. This principle becomes the foundation for understanding how scapular position changes the demands placed on different muscles during climbing movements.
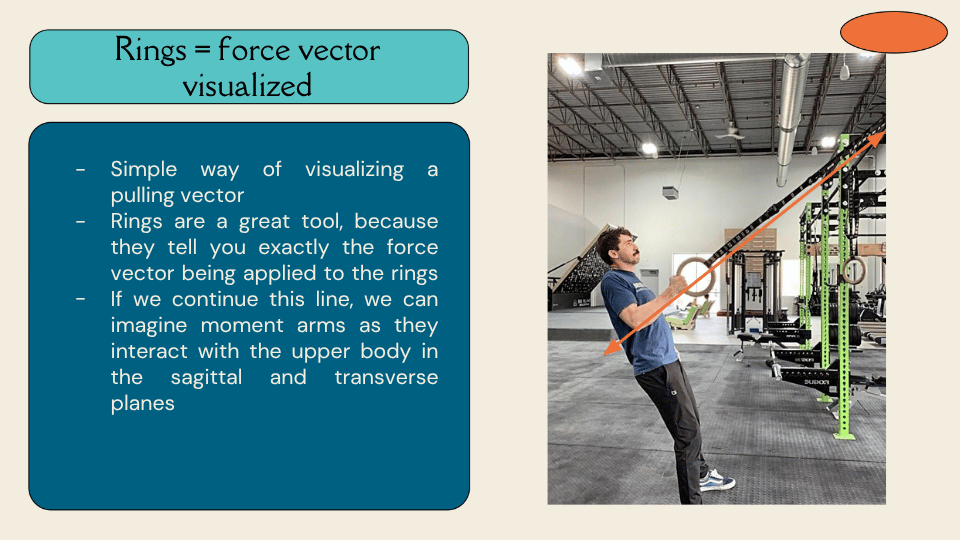
Rings as a Force Vector Visualisation Tool
Gymnastic rings — and by extension, TRX straps — are a useful tool for visualising force vectors, because the strap itself shows you exactly the direction of the force being applied. TH uses this to help patients and clinicians imagine how the line of a pulling force interacts with the shoulder and elbow in both the sagittal and transverse planes. In climbing, a helpful way to think about it is: where would your hand fire to if you let go of the hold right now?
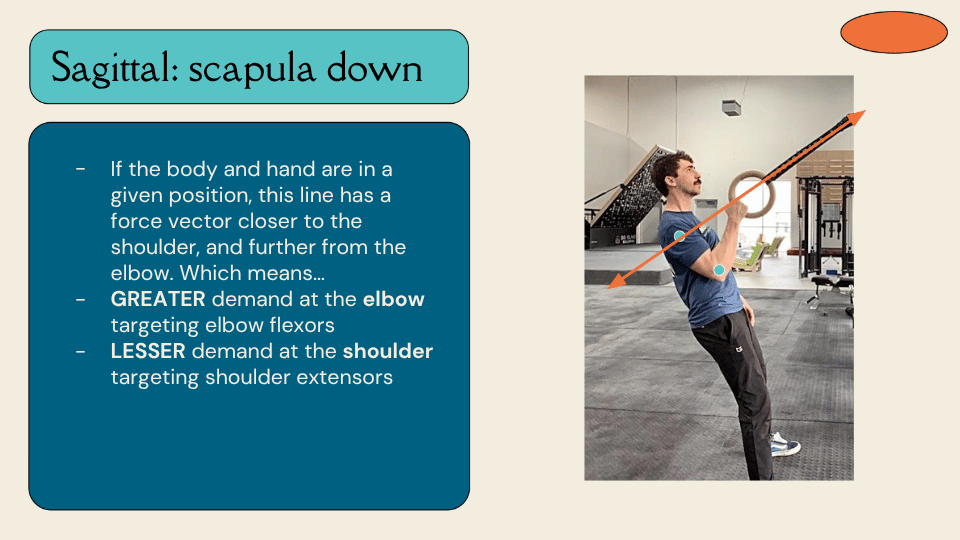
Sagittal Plane: Scapula Down
When the scapula is depressed during a pulling movement, the body and hand position shifts the force vector closer to the shoulder and further from the elbow. The result is greater demand at the elbow targeting the elbow flexors, and lesser demand at the shoulder targeting the shoulder extensors. This is why some climbers feel the effort of a pull almost entirely in their biceps — the mechanics of their position are directing load that way. And if the latissimus is not being called upon as a shoulder extensor in this scenario, TH asks, what is it actually doing? His hypothesis is that it may be functioning as a scapular depressor.
Why Might One Feel This in the Lats?
If the force vector does not create a significant demand for the latissimus as a glenohumeral mover, yet climbers still feel it strongly in their lats during pulling movements, TH proposes that the latissimus may be acting primarily as a scapular depressor in that moment — not as a shoulder adductor or extensor. This is an unstudied hypothesis, but one that he finds clinically compelling and worth investigating.
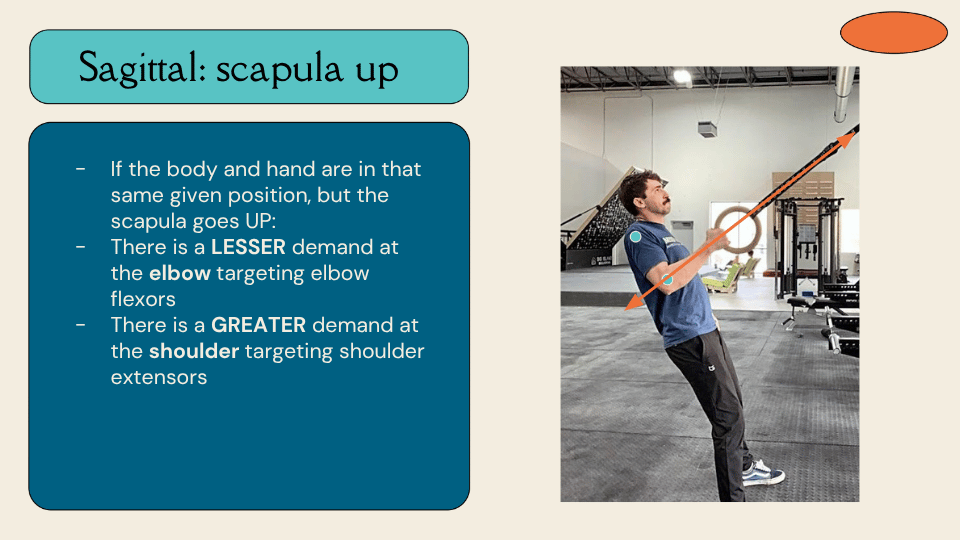
Sagittal Plane: Scapula Up
When the scapula is elevated — a gentle shrug — the same body and hand position produces a different force vector relationship. Now there is lesser demand at the elbow targeting the elbow flexors, and greater demand at the shoulder targeting the shoulder extensors. The pull becomes more shoulder-driven and less bicep-driven. TH notes that even if a climber does not feel the latissimus engaging in this position the way they do in depression, they may actually be getting a more mechanically effective contraction — one that results from the actual force vector being applied, not from the scapula being cranked downward.
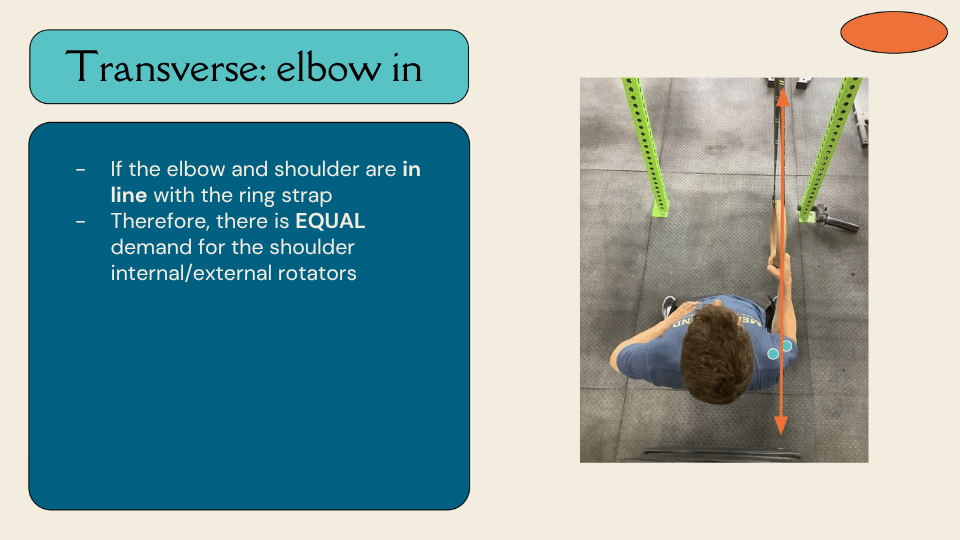
Transverse Plane: Elbow Out vs Elbow In
Viewed from above, the position of the elbow relative to the force vector also matters. When the elbow wings out to the side — a chicken-wing position — the force vector passes medial to the elbow, creating a demand for internal rotation at the shoulder. When the elbow stays in line with the strap or hold, the force vector passes through both the shoulder and elbow equally, creating balanced demand on the internal and external rotators. TH finds that the elbow-in position tends to get the periscapular musculature firing much more effectively.

Bringing It Back to Exam
Armed with this biomechanical framework, TH uses it to inform how he assesses patients. The central question is whether scapular position can give insight into a patient’s ability to produce force. Research already shows that scapular protraction or retraction influences shoulder rotation strength — so there is at least some foundation for this line of thinking, even if the specific application to TOS is not yet studied.
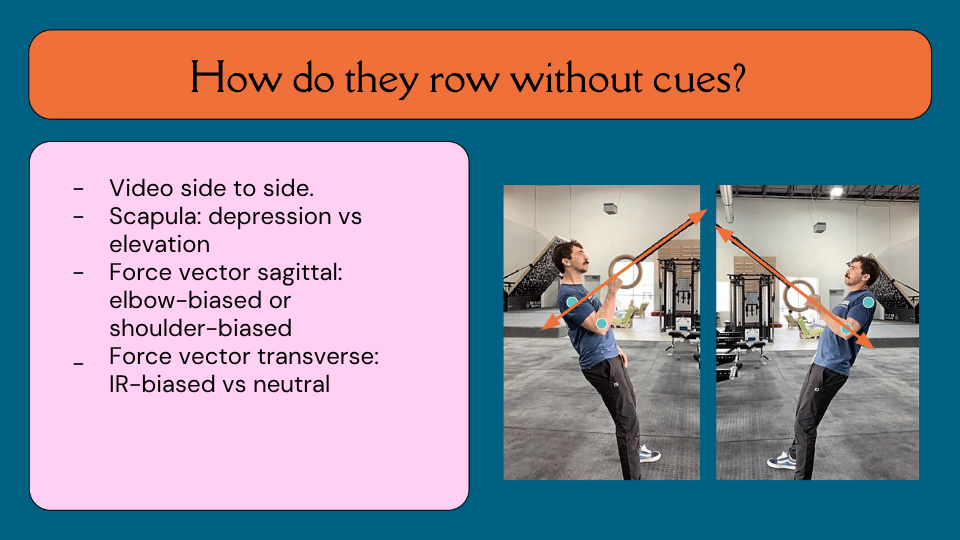
How Do They Row Without Cues?
One of TH’s key assessment tools is watching a patient perform a single or double arm row without any instruction — just to see what their natural movement patterns look like. He videos side to side when he can, and looks for four things: whether the scapula defaults to depression or elevation; whether the force vector is elbow-biased or shoulder-biased in the sagittal plane; whether the elbow tracks in or out in the transverse plane; and whether there are asymmetries between the symptomatic and non-symptomatic sides that reveal a preference for particular motor strategies.
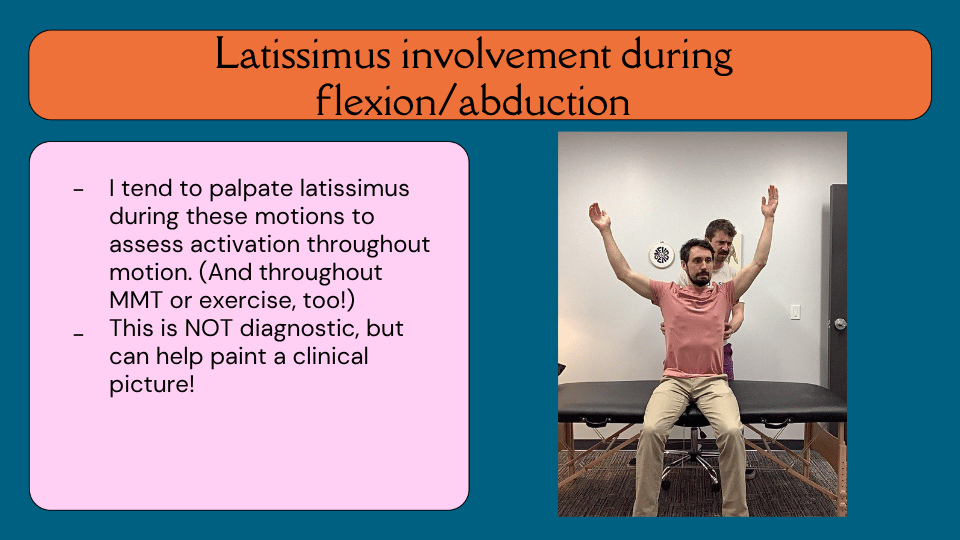
Latissimus Involvement During Flexion and Abduction
TH also palpates the latissimus during shoulder flexion and abduction — movements that should not require significant latissimus activity. If the lat is engaging during these motions, it adds to the clinical picture. He acknowledges the limitation that his hands being on the muscle may itself encourage contraction, but continues to use this assessment alongside manual muscle testing and exercise observation to build his understanding of what the latissimus is doing in each patient.
Scapular Position and Strength Testing
TH takes the clinical observation further by testing external rotation, internal rotation, and abduction strength in both scapular depression and elevation — and comparing results side to side. What he frequently finds is that on the symptomatic side, patients who are strong and confident in depression become uncertain and weak when tested in elevation. They simply do not know how to stabilize or generate force from that position. This asymmetry is not diagnostic, but it is clinically informative and often guides where treatment begins.

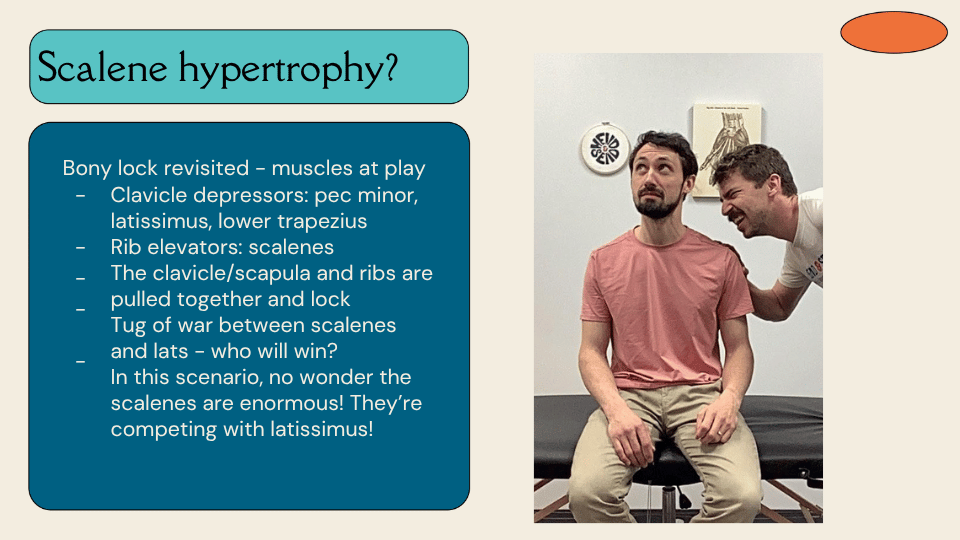
Scalene Hypertrophy
If the latissimus is chronically pulling the clavicle and scapula downward, and the scalenes are simultaneously trying to elevate the first and second ribs, those two muscle groups are engaged in a constant tug of war — and the latissimus is always going to win. From this perspective, scalene hypertrophy is not surprising at all. The scalenes are not the cause of the problem — they are overworked competitors in a battle they cannot win. TH also notes that the upper trapezius, placed on stretch by sustained depression and then loaded under that stretch, is similarly likely to become reactive over time.
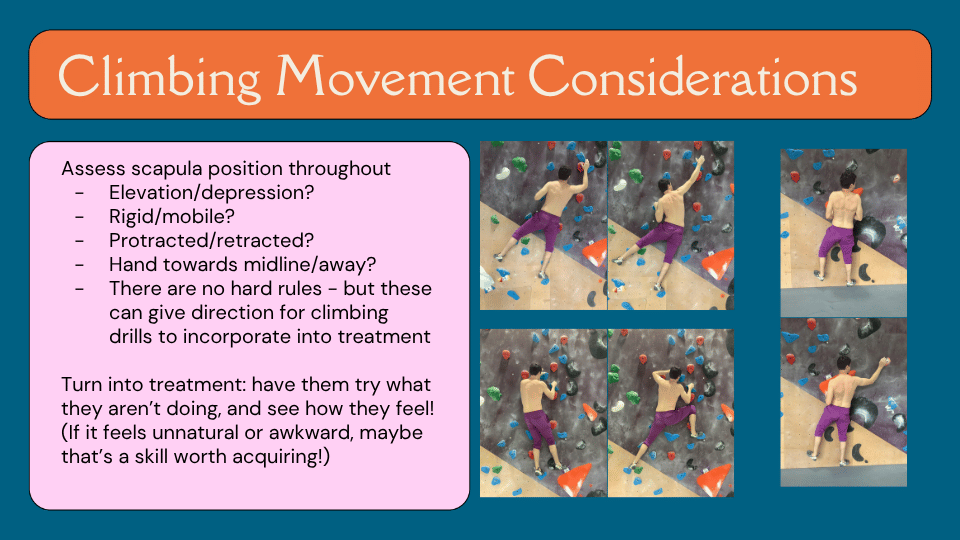
Climbing Movement Considerations: Scapular Position
Because TH works within a climbing gym, he is able to observe patients climbing as part of his evaluation — typically 10 to 15 minutes at the end of the session. He watches scapular position throughout, noting whether it stays elevated, depressed, rigid, or mobile. He looks at whether the hands tend to move toward midline — which reduces the demand on the posterior chain and external rotators — or stay wider. He pays attention to whether one arm moves faster than the other on easy warm-up terrain, which can suggest the climber is not comfortable hanging on one side for extended periods. And he observes drop-knee tendencies, particularly whether they favor one side over the other. None of these observations come with hard rules — but all of them can inform the direction of treatment.
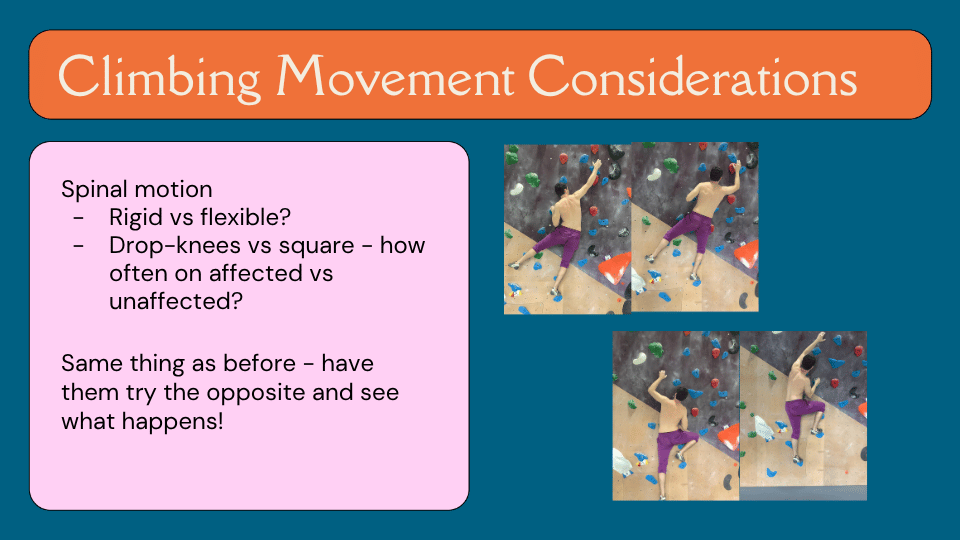
Climbing Movement Considerations: Spinal Motion
TH also watches the spine. Is the climber rigid and square through the torso, or do they have fluid spinal motion? When they pull hard on one side, are they side-bending toward the pulling arm — which would further engage the latissimus connecting the thoracolumbar fascia to the glenohumeral joint — or staying more neutral? Again, neither pattern is inherently wrong. But if a climber is consistently side-bending toward the affected side and depressing the scapula simultaneously, that is a lot of latissimus engagement that may be worth exploring. The treatment approach is simple: have them try the opposite and see what changes.
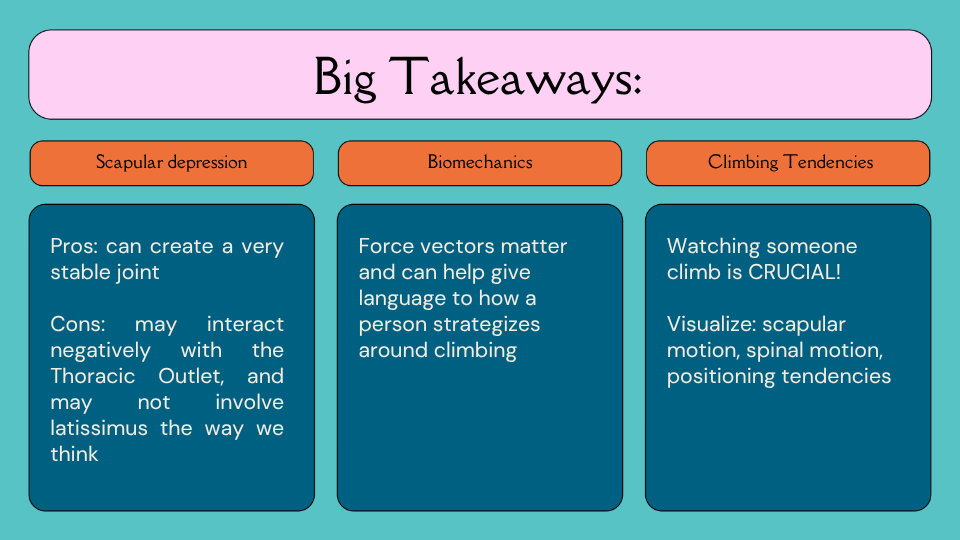
Big Takeaways: Exam Section
Three takeaways from this section. On scapular depression: the pros are reliable joint stability, which is genuinely useful in climbing — especially for hypermobile climbers. The cons are potential narrowing of the thoracic outlet and possible latissimus involvement that goes beyond what we typically account for. On biomechanics: force vectors matter and can give clinicians and patients a shared language for understanding why certain strategies feel intuitive and what the trade-offs might be. On climbing observation: watching someone climb is crucial — and sending videos of easy and hard terrain ahead of an evaluation can give valuable front-end information before the patient even arrives.
Soapbox: Manual Therapy May Muddy the Waters
TH has a candid position on manual therapy in neurogenic TOS: it may make tracking progress harder. Symptom patterns in TOS are already difficult to follow — patients often cannot identify what is making things better or worse, and some sessions are fine while others are not. If manual therapy is introduced alongside exercise, it becomes difficult to know what is actually driving any changes. TH also notes that manual therapy has poor evidence in TOS treatment — Level C at best. His preference is to put the tools in the patient’s hands through education and exercise, so they can observe the relationship between their own strategies and their symptoms.
Patient Education
Because TOS is often the result of a repetitive strategy — a way of moving and loading the shoulder that the body has learned and will likely return to — education is central to long-term management. TH helps patients understand that there are many strategies for achieving shoulder stability, and that the one they have been using has come with a trade-off. Teaching them to experiment with new strategies and track their own symptom responses puts them in control of their own recovery. And if the body has used this strategy once and produced symptoms, it is likely to return to it — which means ongoing self-awareness is part of the long-term plan.
Patient Education: Pain Neuroscience
The pain associated with neurogenic TOS is rarely, if ever, dangerous — which makes pain neuroscience education a powerful tool. TH finds himself saying two things repeatedly to his patients. First: neurogenic TOS pain is a yellow light, not a red light. It is a signal worth paying attention to, not a reason to stop completely. Second: your shoulder is craving stability — let’s help it find a new strategy for getting it, one that does not come with this particular trade-off.
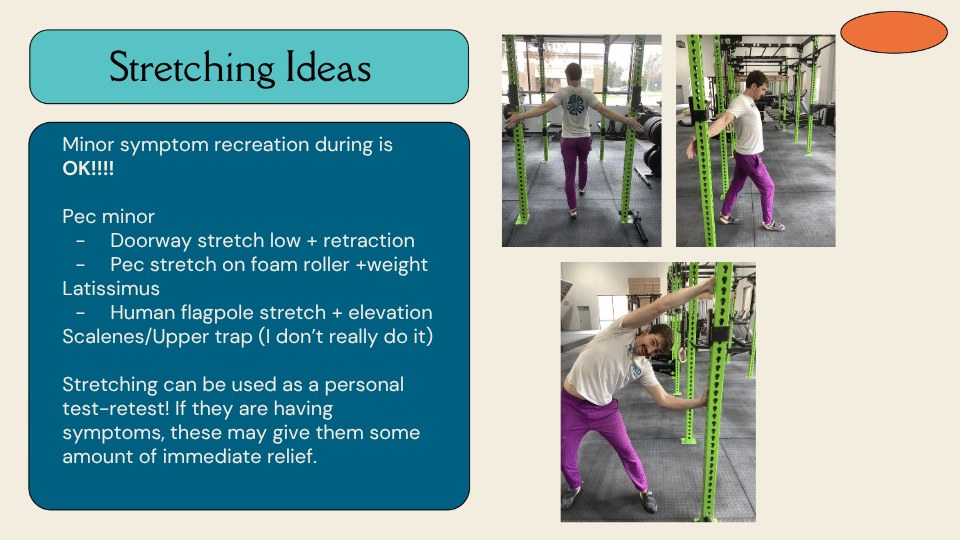
Stretching Ideas
TH is comfortable with minor symptom recreation during stretching — it is not a red flag. For pectoralis minor, he uses a low doorway stretch with an emphasis on scapular retraction and mild elevation, rather than a high doorway stretch that might stress a hypermobile glenohumeral joint. He also uses a pec stretch on a foam roller with light weights, and describes his own experience of staying in that position while symptomatic until the numbness resolved — and then having a completely pain-free climbing session afterwards. For the latissimus, he uses what he calls the human flagpole stretch: standing sideways to a fixed point, pushing the hips away, reaching the arm into full abduction and elevation with contralateral side-bending. He does this while brushing his teeth. For the scalenes and upper trapezius, he generally does not stretch them — his reasoning being that these muscles are likely already being placed on stretch and loaded in that position, and need to be calmed down rather than elongated further. Stretching can also be used as an in-session test-retest: if a climber has a move that is consistently provocative, have them stretch for a full minute and return to see if anything has changed.
Posture: Shrugging
Posture correction in the traditional sense has no strong correlation with pain reduction. But TH offers two practical strategies that patients can use during their day to explore whether position influences symptoms. The first is gentle shrugging when seated — he cues this as gently pinching the shirt tag, so the muscles at the back of the shoulder are contracting at maybe a one out of ten. The second is keeping the elbows under the shoulders rather than flared out. For patients who work from home with adjustable armrests, raising the armrest can passively encourage scapular elevation throughout the day. He also encourages patients to experiment with shrugging versus depressing during tasks they find symptomatic — just to see whether position changes the experience.

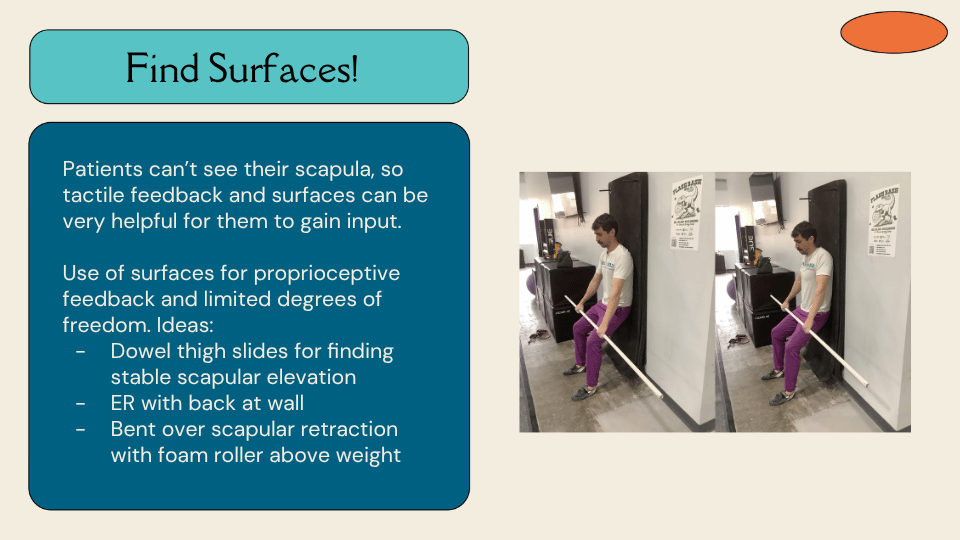
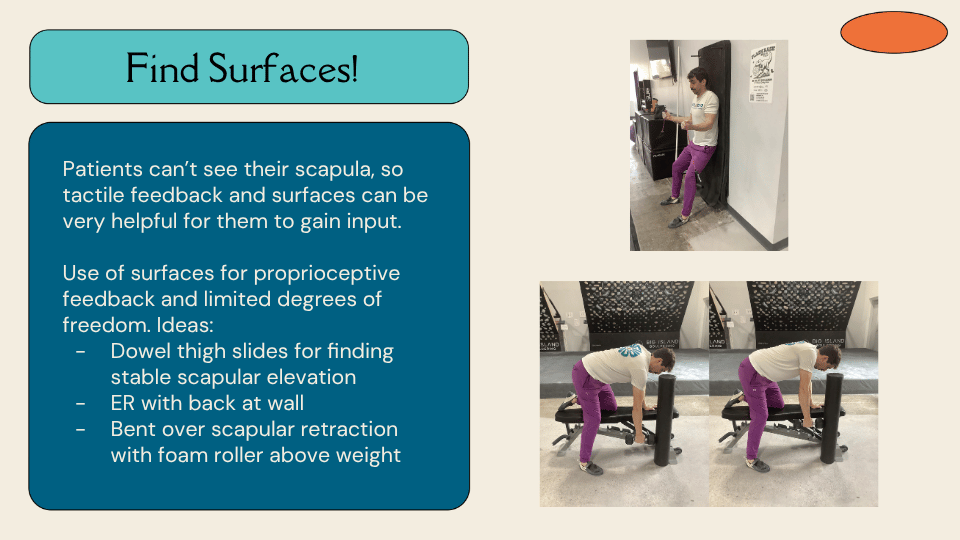
Scapular Proprioception: Find Surfaces
Because patients cannot see their scapula, tactile feedback is essential for helping them find and learn new positions. TH uses three surface-based exercises to build proprioceptive awareness with limited degrees of freedom. The first is dowel thigh slides: seated with the spine supported against a wall, a PVC pipe rests along the thighs, and the patient slides it up and down by gently retracting and elevating the scapulae — inhaling to lift, exhaling to let it drop. The goal is fluid, organic movement with a very gentle contraction. The second is external rotation with the back at the wall: after the dowel slides, patients move straight into wall-supported external rotation to begin building strength in the elevated position. The third is bent-over scapular retraction with a foam roller positioned above the weight: the patient performs retraction while keeping the weight in contact with the roller throughout, preventing the elbow from bending — which would signal the latissimus trying to take over. The foam roller provides a clear visual and tactile cue for what the scapula is doing versus what the glenohumeral joint is doing.
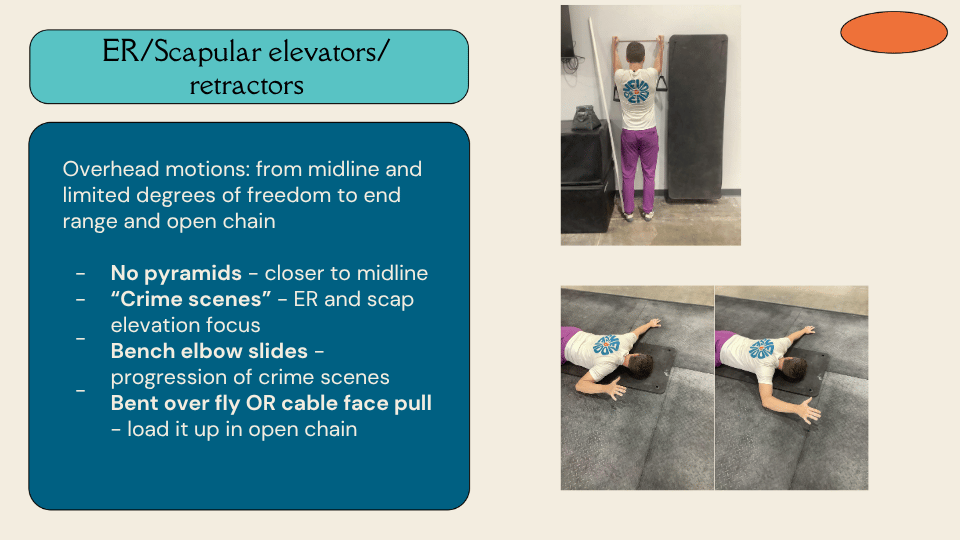
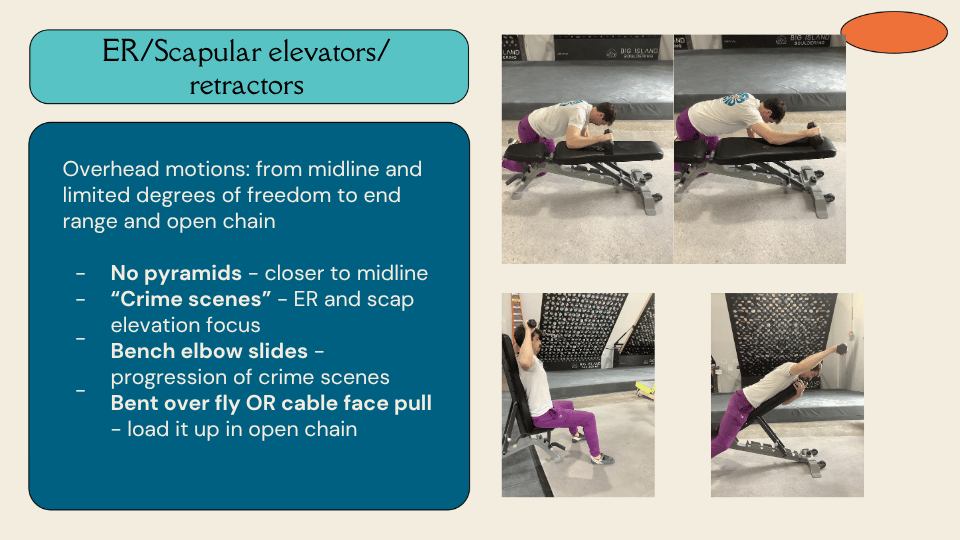
Strengthening: External Rotation, Scapular Elevators, and Retractors
Strengthening progresses from movements close to midline with limited degrees of freedom, toward more open-chain, end-range positions. TH starts with what he calls “no pyramids” — keeping the hands closer to midline where the patient can see them and has more feedback available. From there he moves to “crime scenes” — lying on the floor with one arm out to the side, feet wide, non-working hand pressing gently into the floor for trunk stability, head turned away from the working arm to limit neck involvement. The patient then lifts the hand gently off the floor and uses the surface as a guide to move into abduction and external rotation. The next progression is bench elbow slides: in a quadruped-like position with the elbow resting on a bench, the patient slides up and down in a clean plane of scapular elevation and external rotation. TH notes he has never seen anyone manage more than five pounds with this — it is genuinely challenging. From there, more open-chain options include bent-over flies and cable face pulls with a tricep rope, pulling toward the face and then pressing apart.
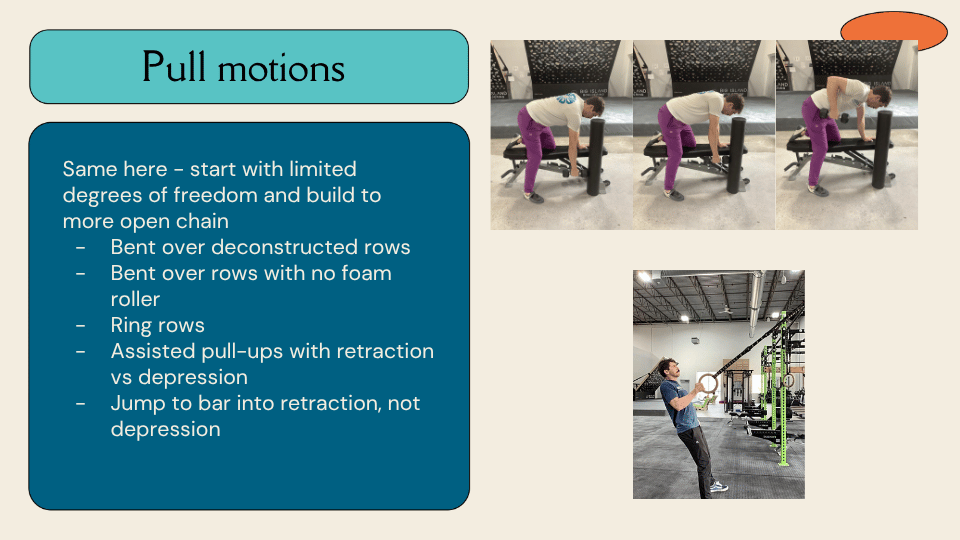
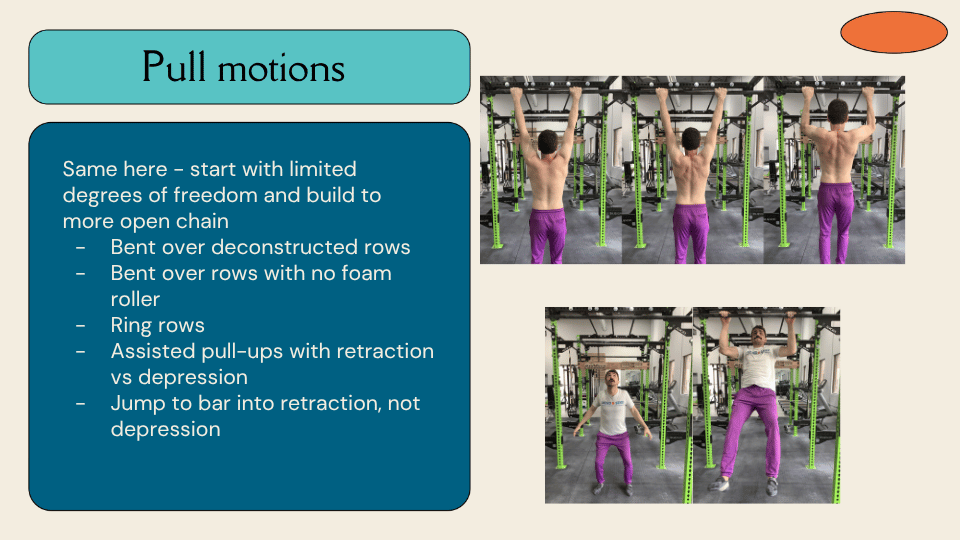
Strengthening: Pull Motions
The same principle applies to pulling — start with limited degrees of freedom and build toward open chain. TH begins with the deconstructed bent-over row with a foam roller, separating scapular retraction from glenohumeral rowing so patients can learn to dissociate the two movements. From there he progresses to rows without the foam roller, then ring rows — where a band around the wrists can be used to encourage external rotation. Assisted pull-ups come next, with a specific cue: bring the shoulder blades toward me, not down. The goal is retraction-initiated pulling rather than depression-initiated pulling. Finally, TH uses a jumping or quick-grab-to-bar exercise where patients learn to stabilize in a retracted position under a brief but aggressive load — varying the degree of shoulder abduction to expose different ranges.
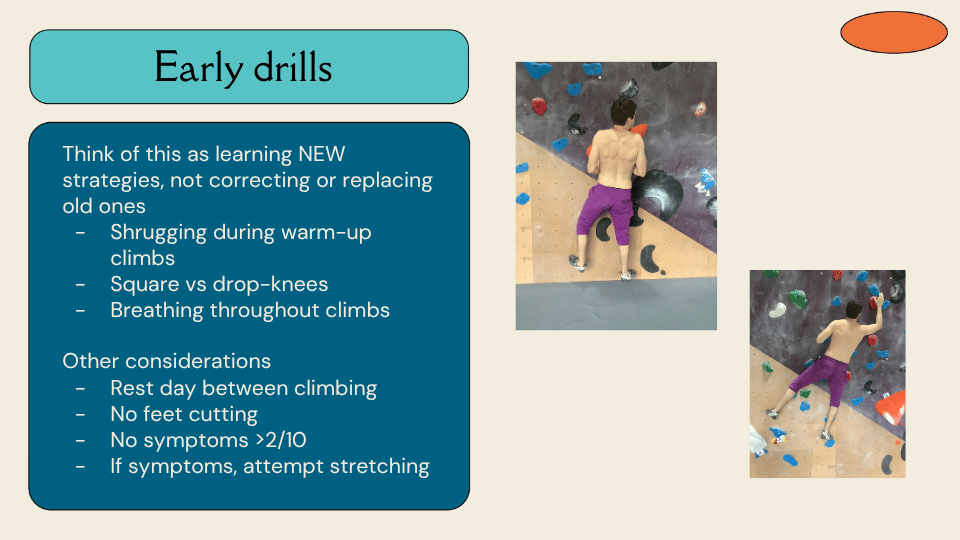
Early Climbing Drills
The framing TH uses for all climbing drills is important: this is about learning new strategies, not correcting or replacing old ones. The goal is to expand the toolbox, not to tell a climber they have been doing it wrong. Early stage drills include shrugging during warm-up climbs — keeping the shoulders gently elevated throughout easy terrain; experimenting with square versus drop-knee positions on the same moves to observe what changes; and paying attention to breathing, particularly whether breath-holding is happening during difficult sequences. Other early considerations include a rest day between climbing sessions, no feet cutting, keeping symptoms below a 2 out of 10, and attempting stretching if symptoms arise during a session.
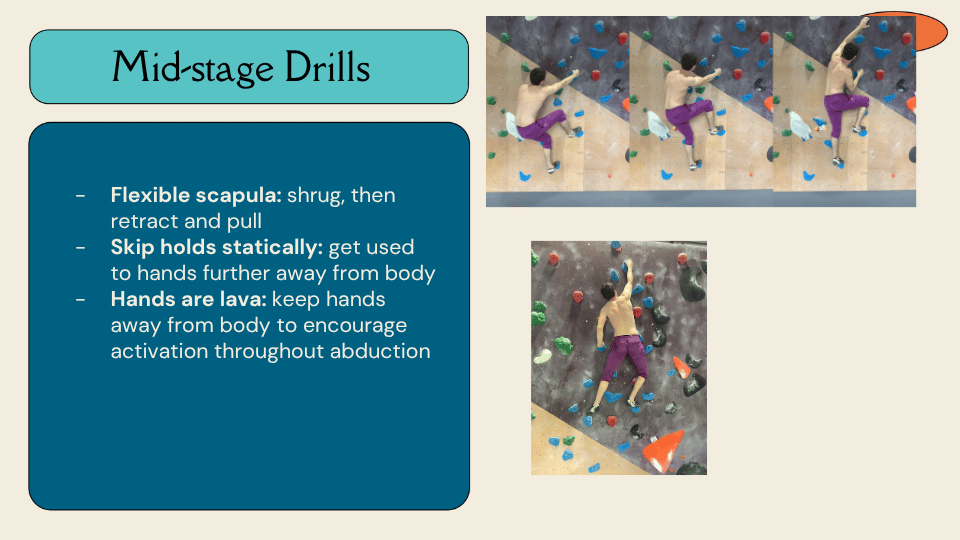
Mid-Stage Climbing Drills
As the climber progresses, TH introduces three mid-stage drills. The flexible scapula drill involves punching the shoulder blade away into protraction before each move, then retracting as the pull happens — building the habit of a mobile rather than fixed scapula. Skipping holds statically gets the climber used to reaching further from their body, spending time in positions where the shoulder is more abducted and the hands are further away. And the “hands are lava” drill keeps the hands away from the body as much as possible throughout a problem — encouraging activation through a wider range of abduction and breaking the habit of pulling everything in toward midline.
Late-Stage Climbing Drills
Late-stage drills reintroduce load and dynamic movement while maintaining scapular awareness. One-foot-on climbing involves choosing one foot to keep on the wall for an entire climb, which introduces gentle feet-cutting and requires the upper body to manage additional load while maintaining position. Peter Pans involve aggressively throwing the legs away between holds — a more dynamic version of feet cutting — while trying to maintain a relaxed, retracted scapular position under a more demanding load. These drills are not corrections — they are stress tests for the new strategies the climber has been building.

Final Thoughts
TH closes with the framework that has come to define how he thinks about this condition. He finds himself approaching neurogenic TOS not as a rigid anatomical diagnosis of irritated structures to be explained and treated pathoanatomically, but as an abstract expression of how a climber uses a biomechanical strategy repetitively — and treating it by helping that climber understand their pain and expand their movement toolbox. The research is frustrating. The diagnosis is elusive. But the approach, in his experience, is far more interesting — and far more useful — for it.
Get in Touch
To connect with TH David or learn more about his work at Mend & Send PT and Performance, reach him at th@mend-and-send-pt.com or follow along on Instagram at @mend_and_send_pt.
References
The clinical insights shared in this presentation are grounded in a growing body of research on thoracic outlet syndrome. The references below include the key literature TH drew on throughout the talk, covering epidemiology, diagnosis, rehabilitation, and biomechanics. Clinicians looking to explore the evidence base further are encouraged to start with the systematic reviews by Garraud et al. on TOS in sport, Luu et al. on exercise rehabilitation for neurogenic TOS, and Dessureault-Dober et al. on the diagnostic accuracy of clinical tests. The current clinical concepts paper by Hock et al. and the literature review by Attaar and Pascarella are also strong starting points for anyone new to this area.
- Disclaimer – The content here is designed for information & education purposes only and the content is not intended for medical advice.

Related Posts