Hypermobility: Strength or Weakness?
How many of us have read an article online, received a pop-up ad on the computer, or even been told by a doctor that we need to stretch more? Odds are, probably most of the population has received this message in one way or another. In a time where yoga and new age stretching studios are all the rage, it seems that flexibility is becoming the key to health, especially for the climber who needs those few extra degrees of hip motion to reach their legs those few remaining inches. But just like many other keys to health that the world promises us, too much of a seemingly good thing can tip the scales in the opposite direction.
Drawing from personal experience, I can think of countless times when my own joint hypermobility has contributed to increased pain not only with athletic endeavors but even everyday activities. As a physical therapy student, I sometimes need to splint or tape my fingers when applying manual massage to a patient to keep these joints in a neutral position to prevent overstretching, an issue I experienced first-hand after tearing the UCL in my thumb. When lifting weights, or playing volleyball, I often tape my wrists to prevent soreness caused by hyperextension. So with this in mind, and considering modern research, is it possible that being hypermobile, or having too much motion in our joints, causes injuries instead of preventing them? I’ll present the facts and let you decide.
What is Hypermobility and How is it Measured?
A person with joint hypermobility may have an excessive range of motion in their joints which allows them to move their limbs into positions that others might not be able to reach. In this condition, the ligaments may be stretched or loose, allowing the bones at joints to move slightly past the limits of their sockets. As you can imagine, this can lead to instability at joints if they are able to move past the ranges where they are most secure. Too much stretching of ligaments can weaken these connective tissues, making injuries like ligament sprains more likely.
It is also important to note the difference from typical muscle lengthening caused by stretching, so consider whether the person is experiencing true ligamentous laxity with joint hypermobility or just increased muscle flexibility. Consider the stretch in a seated position with your legs straight out in front of you where you reach to touch your toes. Is more mobility coming from increased motion at the low back and hip joints or from increased length of your hamstring muscles? As we examine the characteristics of joint hypermobility versus muscle extensibility, we can highlight that the most common hypermobile joints are usually the elbows, wrists, fingers, and knees.1
Joint hypermobility may be accompanied by symptoms which can include but are not limited to joint and muscle pain or swelling which is worse after activity or at the end of the day, stiffness, clicking or popping joints, dislocations, tiredness, and poor balance. There are even some signs and symptoms which may not seem relevant but can point to a potential hypermobility disorder including: upset stomach, digestive issues, bladder and bowel problems, autonomic system dysfunction, easy bruising, poor wound healing, long-term pain, stretchy or soft skin, and chronic fatigue.
When climbing, a hypermobile individual may notice joints like their elbows, knees, and fingers clicking/popping or stretching outside of their normal alignment. Pain may be present in these excessively extended positions and cause difficulty maintaining grip holds. A climber may also become easily fatigued despite being physically strong enough to complete a climb, and take significantly longer to recover than their peers.
Sound like you so far? Let’s continue with some objective measures to be sure. Hypermobility can be assessed through the Beighton Scale, which could indicate hypermobility with a 6/9 in children, 5/9 in middle-age adults, and 6/9 in adults over age 50. This scale assesses hyperextension at the knuckles of both little/pinky fingers, base of both thumbs, both elbows, both knees, and the spine for a total of 9 joints. While a higher score could indicate greater generalized hypermobility, this scale alone cannot diagnose a specific hypermobility syndrome. Similarly, a low score on the Beighton Scale does not necessarily rule out a hypermobility disorder, as hypermobility can also be present with neck, jaw, back, and shoulder pain. It is important to speak with your primary care provider if you have medical concerns involving any of the above signs/symptoms in combination with hypermobility. Even then, medical professionals differ in their interpretation of Beighton Scale results, some of which accept scores <4 as indicative of hypermobility.
But if you’re curious, go ahead and use this infographic from the Ehlers Danlos Society to see how you measure up:

The Research
So, you’ve administered the Beighton Scale and some flags are being raised in your head regarding potential hypermobility. Is this an advantage when it comes to achieving those hard-to-reach climbing positions, or an increased risk for injury?
In a study comparing the type and frequency of injuries among hypermobile and non-hypermobile athletes across different sports, it was found that the overall total number of injuries was greater among the non-hypermobile group.1 These injuries included muscle strains, ligament sprains, dislocations, and bone fractures. Ligament or joint sprains were the most common injury in these non-hypermobile athletes, fractures were equally common in both the hypermobile and non-hypermobile, while joint dislocation was experienced only by hypermobile individuals.1 From this specific study, we can gather that it is more likely for a hypermobile athlete to suffer a joint dislocation but less likely for them to experience a ligament or joint sprain. This makes sense because an athlete whose ligaments are over-stretched and lax is already in a vulnerable position where it could take the slightest stress to push the joint out of position. However, it is less likely for them to experience a severe ligament strain because the ligaments are already in a stretched position. For example, a hypermobile athlete rolling their ankle would be less likely to result in a sprain because their ankle can already reach this greater range of motion naturally, compared to a non-hypermobile athlete whose ankle is being forcefully stretched into this range, resulting in ligament injury.
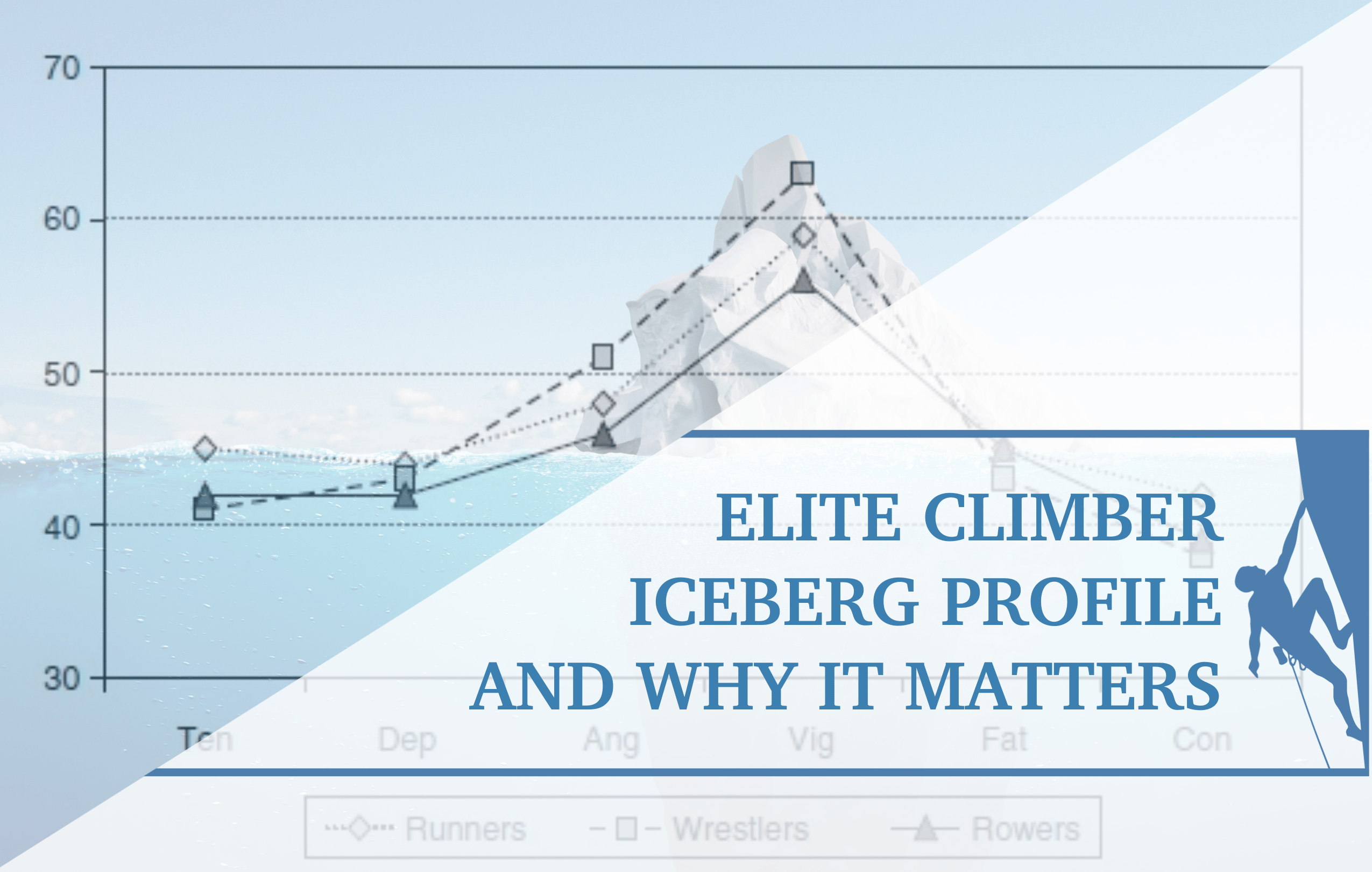
Another study assessed physical characteristics of elite climbers, one of which was range of motion at the hip joints.2 When discussing hip joint flexibility in climbers, leg span is an important quantitative measure. These researchers found that leg span measured 139 ± 4 cm in elite climbers, 122 ± 4 cm for recreational, and 124 ± 4 cm in non-climbers.2 This means that the elite climbers had the greatest average leg span, so they demonstrated more hip flexibility than both recreational and non‐climbers.
A second study examining the physiological characteristics of elite climbers concurred with this group of researchers and named flexibility as one of four main abilities that determine climbing success.3 They asserted that climbers need to be able to lift their legs high, rotate significantly, and reach out wide while maintaining control of the body in extreme positions. For these reasons, the researchers specifically highlighted hip joint range of motion as having a positive impact on climbing performance while also recognizing that hypermobility of the hips can also damage these joints.3 It is possible that increased motion at the hip joint can stretch out ligaments or put the joint in vulnerable positions that are less stable, making it difficult for climbers to even maintain these far-out holds.

Image showing hip flexion and external rotation pattern necessary for climbers, in the context of a test designed to measure these movements.3
Still, more researchers out there are asserting that flexibility is crucial for sport climbers and have channeled their efforts into designing climbing-specific measures of this unique flexibility which these athletes must demonstrate.4 They believe that designing tests unique to rock climbers will better identify the proper joint range of motion for reducing injury and raising performance in this sport.4 It seems that the question of hypermobility may have a conditional answer that isn’t so black and white, but rather something like “it depends”. Some studies show that hypermobility doesn’t always result in more injuries, while others suggest that it contributes to an increase in certain types of injuries but prevention of other specific types.
Unfortunately, there isn’t much research out there involving the relationship between climbing-specific injury risk and hypermobility but there is extensive research on other sports. In a study that classified 139 professional football players as either “loose” or “tight” based on joint mobility, there was an increased likelihood of knee ligament rupture among those classified as having looser joints.5 Studies involving Division I rugby players6, junior netball players7, and a meta-analysis of generalized contact-sport athletes8 also found a strong positive relationship between higher Beighton Scale scores and increased injury risk. Still, other studies offer conflicting or inconclusive results, suggesting that there may be no significant difference in overall injury rates between hypermobile and non-hypermobile male professional soccer players9 or lacrosse players10.
Could it be that the risk of injury in hypermobile versus non-hypermobile athletes depends on the sport? This would call into question a variety of factors from playing surfaces to environmental conditions, level of contact, common movement patterns, and physiological differences between athletes of these various sports. All the more reason to call for action in generating research on hypermobile athletes in the sport of climbing. We know that many elite athletes are hypermobile, especially when it comes to sports where increased mobility may be advantageous, like climbing. However, there are greater considerations for health maintenance and injury prevention in these individuals. So, you can argue that hypermobile athletes are less prone to something like ligament strains or muscle sprains because they already have greater movement within the joints such that a large shift may not cause the damage that it would to a non-hypermobile individual.

However, hypermobile athletes could have more dislocations because their ligaments could already be in a vulnerable state since increased laxity is already present, thus decreasing control of the joint. Using this image as an example of ankle inversion, a normal person would likely experience some sort of ligament injury in this over-stretched position, while a hypermobile individual may not experience discomfort if their ankle is naturally able to reach this range of motion.13
These athletes could also be more prone to tendinopathies, tendonitis, and tendinosis, and take longer to recover from such injuries. In the study involving professional soccer players, hypermobile athletes missed more training sessions and games during the course of their injuries than less mobile teammates, but the difference was not considered statistically significant.9 In another professional soccer study, hypermobile players had a greater number of injuries and were more likely to have a severe injury, recurrence of injury throughout the season, and miss more days of training or games11.
But no matter which research article or thesis you choose to follow, the bottom line appears to be this: joint range of motion and flexibility are essential to success in rock climbing. Now we just need to explore how to accomplish this safely.
See a Doctor of Physical Therapy
Physical therapists are movement specialists trained in the art of injury prevention and rehabilitation. Contrary to popular belief that PT actually stands for “physical torture”, their methods are actually intended for good, and many of these doctors specialize in sports injury. It may be worth consulting a physical therapist for a specific diagnosis of the aches and pains you’ve just been pushing through. Even if you think nothing is egregiously wrong, it can be helpful to simply ask questions to gain insight or boost your sports performance. After administering diagnostic tests for hypermobility and injury identification, physical therapists can apply manual therapy, physical exercise, mobility techniques, pain-reducing modalities, and other various treatment methods to promote a safe return to sport. The images and videos below depict a few of these diagnostic tests and exercises relevant to rock climbers.
Tests for Hypermobility or Joint Instability
To give you a little taste of what you might experience if you consult a physical therapist with concerns of hypermobility, here are a few special tests they may perform.
Shoulder Anterior Apprehension (Crank) Test
This is a physical exam to determine whether a patient may have shoulder instability or a dislocation. The patient lies on their back, and the therapist bends their elbow to 90° while also raising their arm out 90° to the side. The therapist then slowly rotates the arm backward while monitoring the patient for signs of apprehension or fear of dislocation. While the patient may experience pain with this maneuver, pain alone does not necessarily indicate a positive result. The goal is to assess whether there is laxity or injury to the ligaments in the front of the shoulder, contributing to hypermobility.
Hip Prone Instability Test
Micro-instability of the hip can have traumatic or atraumatic cases related to repetitive axial or rotational loading combined with joint structural abnormalities, labral tears, joint capsule laxity, ligament injury, or muscle dysfunction. For this test, the patient lies on their stomach while the therapist bends one of their legs to 90° at the knee so the foot is facing straight up at the ceiling. The therapist then pushes down on the greater trochanter (upper part of the posterior thigh just wide of the glutes) of the hip being tested and externally rotates the patient’s hip. Pain in the front of the hip with this maneuver indicates a positive result and can suggest hip instability due to hypermobility of the joint.
Patellar Apprehension Test
Instability of the patella, or kneecap, due to laxity of the medial patellofemoral ligament or cartilage defects can contribute to lateral dislocation. While dislocation is often traumatic in nature, hypermobility of the patella makes this injury more likely. The patellar apprehension test assesses the risk of instability and dislocation. The patient is usually seated with their leg extended straight out in front of them. The therapist uses their thumbs to press on the medial side of the patella to apply pressure that pushes the kneecap laterally. A positive test result includes verbal, visual, or physical expression of the patient’s fear that the patella might dislocate; the patient may tense up their leg and contract their thigh to bring the patella back into alignment or attempt the stop the therapist from pushing it further.
Anterior Drawer Test for Chronic Ankle Instability
Laxity of the ligaments in the front/lateral side of the ankle can make athletes prone to rolling and spraining this joint. This test assesses the strength of mainly the anterior talofibular ligament (ATFL) by stabilizing the leg and pulling the foot forward to determine if there is excessive forward motion. The patient lies on their back with the knee of the tested leg slightly bent. The therapist then holds down the lower leg just above the ankle with one hand and uses the other hand to point the patient’s foot slightly downward. The therapist then gently pulls the foot forward from the heel and assesses whether a gap appears on the front/lateral side of the ankle or if there is increased forward motion.
Strength Exercises for Controlling Hypermobility
While ligaments provide a more taught, passive form of stability at joints, muscles provide a more dynamic form of stability. Muscle contractions control the motion of bones around a joint, so strengthening them can help control hypermobility in people whose ligaments are more extensible in order to increase the support. This can essentially provide a secondary form of bracing to maintain joint positions in optimal alignment. The following are exercises designed to strengthen the muscles surrounding the fingers, wrist, shoulder, hip, knee, and ankle joints.

Finger/Hand Strength: Ball Squeezes
Strengthening the inner muscles of the hands and fingers can improve control of grip, which is often lost when the fingers are in a hyperextended position. Grasp a stress ball with the palm and fingers and squeeze for 10-20 seconds as many times throughout the day as possible without pain or excessive fatigue. It is important to keep the fingers within a neutral range while performing these squeezes, so the joints are not further stressed.


Shoulder/Arm Strength: Push-Ups (Full and Modified/Knee)
This is a great exercise for strengthening the shoulder, upper back, core, and muscles surrounding the elbow. When bending the arms to lower down, be sure to stop with the elbows at 90° to avoid pushing the shoulder joints too far forward. Also, refrain from locking the elbows out into full extension at the top of the exercise so as to not stress the joints in a hyperextended position. This exercise can be performed with the legs fully extended propped up on the toes or modified on bent knees, but the core muscles must be tightened and trunk fully straight. Try 3 sets x 10 reps or until fatigue.

Hips and Core Strength: Bird-Dog
This exercise increases core activation with hip, glute, and shoulder muscle strength within a controlled range of motion for improving postural control and balance. Position yourself on hands and knees, then raise one arm and the opposite leg up extended out in a straight line with your body. Hold this position for 2-3 seconds, then relax back down onto hands and knees, and perform with the opposite arm and leg. Complete 2 x 10 each side or until fatigue. Be sure to tighten your core muscles to provide greater stability.

Quadriceps/Glute Strength: Squats
Improving strength of the leg and hip muscles can relieve stress placed on the knees. To make this exercise specific to climbers, you can externally rotate your hips and distance your feet further apart for a sumo squat stance. It is important to bend and straighten the knees slowly, and avoid locking them out into full extension, so as to challenge the muscles without stressing the joint. Also, make sure to bend your knees just until your kneecaps are in line over the toes and not past them. This improves control within a normal range of motion. Try 3 sets x 10-12 reps or until fatigue.
Lower Leg/Ankle Strength: 4-Way TheraBand Exercises
Strengthening the lower leg muscles will give them better control of the ankle joint to prevent injury from sprains. This exercise is often performed in a seated position with both hands holding one side of the TheraBand, while the other side is looped around the foot. The four directions include dorsiflexion (toes pointing up towards your nose), plantar flexion (pointing toes down to the ground), inversion (bottom of foot pointing towards the midline of the body), and eversion (bottom of foot pointing laterally away from the body). Complete 2 sets x 10 reps in each direction and increase the resistance of the band when the exercise feels too easy.
Let’s bring it all together. Research shows that increasing flexibility and range of motion at joints gives elite climbers an advantage over those who cannot get into those difficult-to-reach positions. But it also suggests greater injury rates among hypermobile individuals, especially related to ligament sprains and joint dislocations. So, maybe the question isn’t about whether hypermobility is a strength or weakness as it relates to rock climbing, but rather how it can best be controlled to improve performance while reducing injury risk. Again, this is where it may come in handy to consult a physical therapist for proper exercise prescription based on your individual needs. Strengthening the specific muscle groups involved in limb motion can improve control of structural support if the exercises are performed within a safe range that does not push the joint outside its normal limits. by increasing muscular strength, you can reduce the strain placed on joints in certain positions. These exercises not only improve joint stability, but they can increase balance, relieve pain, and enhance posture. Below are a few examples of exercises which can help hypermobile and non-hypermobile individuals alike to improve control in end-range positions.
Since joint range of motion isn’t the only contributor to mobility, it is important to address how to safely stretch muscles because the increased length can be advantageous, too. Chances are, if you are hypermobile, then deep stretching may not be as appropriate for you. This is why it is important to consult your doctor or physical therapist about the nature of your hypermobility, and which activities are recommended.
Below are a few examples of relevant exercises for climbers to perform after training or competition because these are static stretches intended to increase muscle length and reduce stiffness. It is not ideal to perform these specific exercises prior to training or competition because preserving a certain amount of muscle stiffness for these activities can improve muscular strength and control for preventing hyperextension of joints. Prior to activity, it would be more beneficial to warm up using low-impact cardiovascular exercise such as cycling, walking, or light jogging combined with dynamic mobility drills such as high-knees, skipping, heel kicks, or walking straight leg raises.
Static stretches are more beneficial when performed after activity because the muscles are warm and more prone to lengthening. Notice how in the static stretches below, the positions are achieved with slow control and held in the same form throughout. Avoid bouncing or dropping quickly into position to reduce the risk of muscle or joint injury. Hold each stretch for 2 x 30 seconds at mild discomfort. You should feel a deep stretch, but not an increase in pain.
Proper stretching to increase safe mobility: 2-3 exercises
Use the videos below for examples of how to execute common stretches properly while staying within a safe, stable range of motion and not stressing the joints.

Standing Quadriceps Stretch
Stand on one leg while bending the opposite leg behind you, hold it there with one or both hands to ensure that it is aligned vertically parallel to your standing leg. Do not pull your foot to the right or left side because this will rotate the leg, placing stress on the knee joints instead of lengthening the targeted muscle. Hold this stretch for 2 x 30 seconds on each leg.

Ankle Dorsiflexion Wall Stretch
Stand with one foot flat on the ground about 3-5 inches away from the wall and the toes of the opposite foot inclined up against the wall with the heel of that same foot on the ground. While keeping your legs straight, lean your body towards the wall until you feel a stretch of mild discomfort in the calf muscle of the leg which is pressed against the wall. Hold this stretch for 2 x 30 seconds on each leg. Be sure not to hyperextend the knee of the leg that is being stretched, so as not to injure the ligaments of the knee. If this stretch feels too easy, slightly bend the knee of the leg being stretched and lean closer to the wall while keeping the heel in contact with the ground.

Doorway Chest/Shoulder Stretch
To stretch the muscles below your shoulder and increase your vertical reach, place one or both hands on the top of a doorway and take one step forward or lean into the doorway. To stretch the muscles in the front of your shoulders and chest for increasing lateral reach, raise one or both arms out to the sides with your elbows bent to 90° and step forward or lean into the doorway. Hold each stretch for 2 x 30 seconds and avoid over-stretching your shoulders backward such that your shoulder bones “pop” forward, as this can stress the ligaments in the front of the shoulder. Hold each stretch at a point of mild discomfort.
Moving Forward
Okay, it’s decision time. The facts have been presented and recommendations have been made. Now it’s time for you to decide your course of action. Maybe you’ve attempted the Beighton Scale or considered your symptoms and are now raising some questioning flags in your mind as to whether you might potentially be a hypermobile athlete. You’ve been experiencing pain, excessive fatigue, or discomfort and want to know how to better control your mobility to reduce injury risk. Or maybe you’re on the opposite end of the spectrum with individuals needing to increase mobility to enhance their climbing performance. So, what do you think: is hypermobility a blessing or a curse? Either way, it’s important to consult a medical professional if you have concerns so you can receive proper treatment and become the best athlete you can be.
In the meantime, you can make simple lifestyle modifications to generally improve your health by getting enough sleep, consuming a healthy diet, staying hydrated, and not self-manipulating or cracking your own joints. Cross-training with low-impact activities such as cycling or swimming are also beneficial because they challenge different muscle groups while placing less stress on the joints, thereby reducing pain and improving function. While continuing to climb, learn the ranges in which your joints are most stable and try to remain within them. You can watch videos or have someone else provide feedback on your positioning from a different perspective. Braces or tape may even be helpful for joints you have difficulty controlling, such as the fingers or wrist. Also, be sure to complete a thorough warm-up with gentle, dynamic mobility exercises that do not excessively stretch the joints.
Listen to your body!! Realize that it is sometimes more beneficial to take a rest day to recover and heal your body than to strain yourself by incorporating more training. Reduce your climbing volume or number of attempts on the same course if you need to. Be intentional when scheduling rest days and hold yourself accountable. Whether or not you are hypermobile, these are important principles to live by when navigating a sport as demanding as climbing because fatigue and injury can be so impactful. Remember, to consult a medical professional if you have concerns before spiraling into the trap of self-diagnosis. Be aware and become informed.
And feel free to share your questions, comments, and personal anecdotes with the climbing community in the comments below. We’d love to join you in your mobility journey!
Author Bio
Emily Leonard is a third-year Doctor of Physical Therapy Student (SPT) at the University of Florida with a Bachelor of Science degree in Biology with minors in Chemistry and Spanish from Mercer University. Her career goal of becoming a Sport-Certified Specialist in Physical Therapy is driven by personal experiences as a former Division I Beach Volleyball player and the empathy she shares with athletes undergoing the rehabilitation process to return to sport. Emily’s interest in rock climbing began when a recreational sport climbing gym opened up in her college town and captivated the interests of her friend group. By no means an expert climber herself, Emily has taken to research to understand how she can apply her knowledge of physical therapy to this new arena of sports.

She is currently certified in CPR/AED + First-Aid Basic Life Support and Emergency Medical Response (EMR) and is a Certified Strength and Conditioning Specialist (CSCS). In her free time, Emily enjoys playing beach volleyball and soccer, watching football, working out at the gym, taking her dog to the park, hiking, camping, and spending time with family and friends.
Reach out to Emily via email with questions or further discussion: eleonard@ufl.edu
Resources:
- Nathan, J. A., Davies, K., & Swaine, I. (2018). Hypermobility and sports injury. BMJ open sport & exercise medicine, 4(1), e000366. https://doi.org/10.1136/bmjsem-2018-000366
- Grant, S., Hynes, V., Whittaker, A., & Aitchison, T. (1996). Anthropometric, strength, endurance and flexibility characteristics of elite and recreational climbers. Journal of Sports Sciences, 14(4), 301–309. https://doi.org/10.1080/02640419608727715
- Draga, P., Ozimek, M., Krawczyk, M., Rokowski, R., Nowakowska, M., Ochwat, P., Jurczak, A., & Stanula, A. (2020). Importance and Diagnosis of Flexibility Preparation of Male Sport Climbers. International journal of environmental research and public health, 17(7), 2512. https://doi.org/10.3390/ijerph17072512
- Nick, D., Brent, S., Hodgson, C., & Blackwell, G. (2009). Flexibility assessment and the role of flexibility as a determinant of performance in rock climbing. International Journal of Performance Analysis in Sport. 9. 67-89. 10.1080/24748668.2009.11868465
- Nicholas JA. Injuries to knee ligaments: relationship to looseness and tightness in football players. J.A.M.A. 1970; 212: 2236–9.
- Stewart DR, Burden SB. Does generalised ligamentous laxity increase seasonal incidence of injuries in male first division club rugby players? Br. J. Sports Med. 2004; 38: 457–60. doi:10.1136/bjsm.2003.004861
- Smith AK, Damodaran S, Swaminathan R, et al. Hypermobility and sports injuries in junior netball players. Br. J. Sports Med. 2005; 39: 628–31. doi:10.1136/bjsm.2004.015271
- Pacey V, Nicholson LL, Adams R, Munn J, Munns CF. Generalized joint hypermobility and risk of lower limb joint injury during sport : a systematic review with meta-analysis. Am. J. Sports Med. 2010; 38: 1487–97. doi: 10.1177/0363546510364838.
- Collinge R, Simmonds J. Hypermobility, injury rate and rehabilitation in a professional football squad — a preliminary study. Phys. Ther. Sport. 2009; 10: 91–6
- Decoster LC, Bernier JN, Lindsay RH, Vailas JC. Generalized joint hypermobility and its relationship to injury patterns among NCAA lacrosse players. J. Athl. Train. 1999; 34: 99105
- Konopinsy MD, Jones GJ, Johnson MI. The effect of hypermobility on the incidence of injuries in elite-level professional soccer players: a cohort study. Am. J. Sports Med. 2012; 40: 763–9. doi:10.1177/0363546511430198
- Baeza-Velasco, Carolina MA, PhD; Gély-Nargeot, Marie-Christine PhD; Pailhez, Guillem MD, PhD; Vilarrasa, Antonio Bulbena MD, MSc (Cantab). Joint Hypermobility and Sport: A Review of Advantages and Disadvantages. Current Sports Medicine Reports 12(5):p 291-295, September/October 2013. | DOI: 10.1249/JSR.0b013e3182a4b933
- Introduction to Joint Hypermobility. Physio Elements. December 03, 2020. https://www.physioelementsny.com/blog/2020/12/04/introduction-to-joint-hypermobility-and-connective-tissue-disorders/13
- Disclaimer – The content here is designed for information & education purposes only and the content is not intended for medical advice.

Related Posts