Case Study: PT Management of a Rock Climber with Talar Neck Fracture
In this engaging presentation, Dr. Allison Tran, a physical therapist and a board-certified orthopedic clinical specialist, presents a case study on managing a talar neck fracture in a rock climber. This session outlines the injury background, surgical interventions, and a comprehensive rehabilitation plan focused on returning to climbing. Dr. Tran’s expertise guides viewers through the stages of tissue healing, strengthening, stability optimization, and sport-specific training, highlighting the complexities of treating ankle injuries in active climbers.
Topics Covered:
- Background and surgical history of the talar neck fracture
- Key rehab phases for safe return to climbing
- Techniques for maximizing ankle mobility and strength
- Sport-specific drills for climbing and high-impact activities
Learning Objectives:
- Understand the progression from acute care to return-to-sport after a severe ankle injury
- Learn specific interventions to improve ankle function for climbers
- Gain insights into sport-specific modifications for a safe return to climbing
Introduction
This case study details the rehabilitation journey of a 36-year-old male trad climber who sustained a talar neck fracture. Through a structured physical therapy approach, the case highlights challenges in recovery and the pathway back to climbing.

Case Background
The climber sustained a serious injury from a 15-foot fall, resulting in a displaced, comminuted talar neck fracture and subtalar joint (STJ) dislocation. Delayed evacuation led to compartment syndrome, necessitating urgent surgery.
The climber’s initial surgeries included decompression, stabilization, and open reduction internal fixation (ORIF) of the talar neck. After three months of consistent physical therapy, he embarked on a year of intermittent therapy due to travel, but continued to experience pain that limited his climbing activities.
Case Background – Third Surgery
The climber underwent a third surgery for hardware and osteophyte removal, along with scar tissue debridement. An MRI revealed post-traumatic degenerative changes in the STJ, bone edema in the talus, and chronic sprains, complicating his recovery.

Subjective Evaluation
At 2.5 months post-surgery, the climber reported ongoing pain, stiffness, and swelling in the ankle, worsened by activities like prolonged walking, hiking, and climbing. His primary goal was to regain the ability to hike and climb without pain.
Current Activity
The climber’s sporadic physical therapy focused on basic ankle exercises like calf raises and resistance band work, but he reported feeling unmotivated and isolated from his passion for climbing, noting that “climbing was my life.”

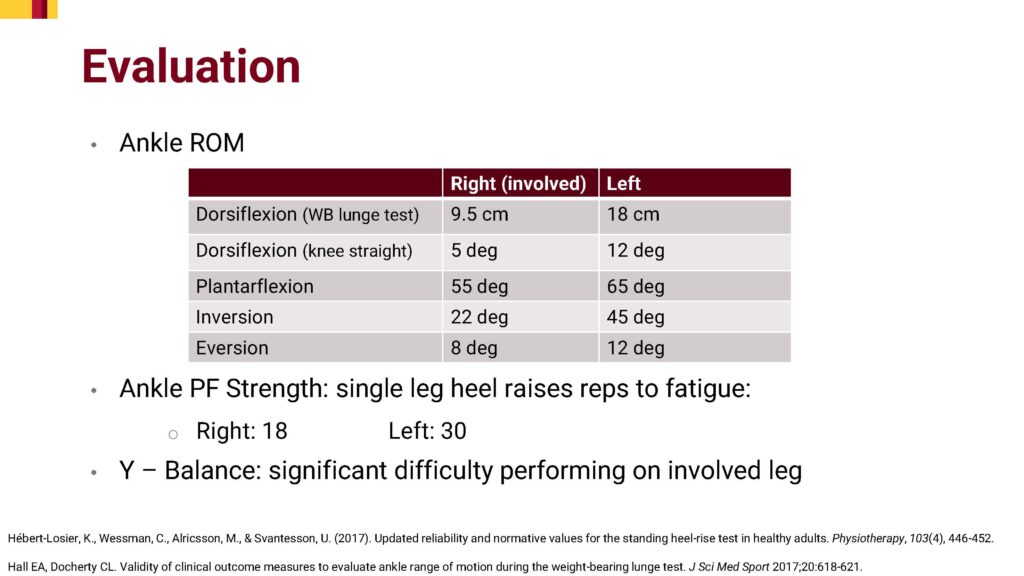
Objective Evaluation
An assessment revealed limited range of motion, strength deficits, and instability in the injured ankle. Tests like the Y-Balance Test indicated significant difficulty with balance and strength on the affected leg, emphasizing the need for targeted interventions.
Return-to-Sport Progression
The rehabilitation progression plan involved phases aimed at tissue healing, mobility, strength, stability, and eventual return to climbing, ensuring a gradual and supported pathway back to physical activity.

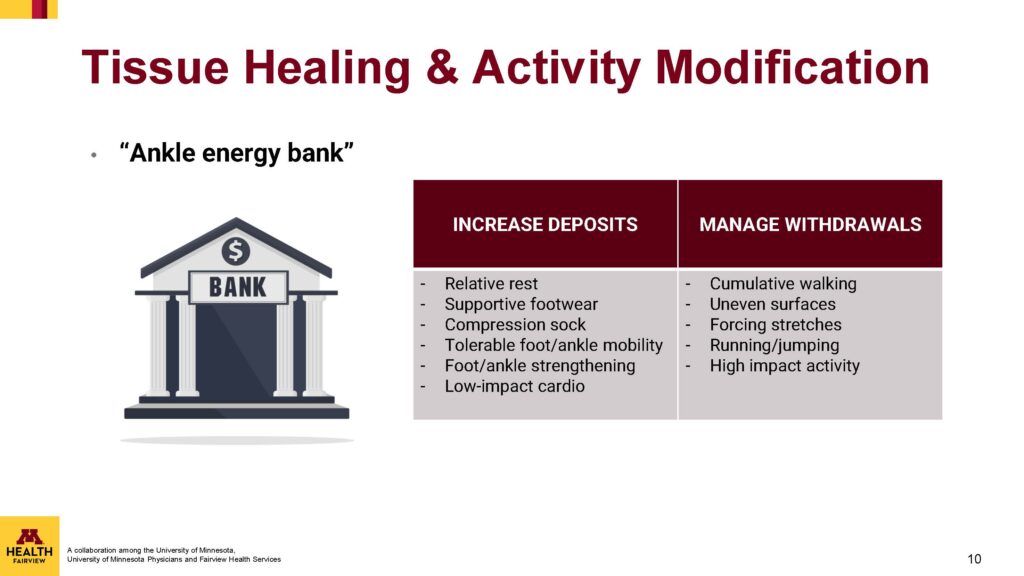
Tissue Healing and Activity Modification
Using the concept of an “ankle energy bank,” the climber was advised to balance “deposits” (activities that promote healing, like low-impact cardio and supportive footwear) and “withdrawals” (high-impact activities or uneven surfaces that could hinder recovery).
Improving Range of Motion
Manual therapy focused on joint mobilizations, especially for the talocrural and subtalar joints, and soft tissue work around surgical scars and the calf muscles. A home exercise program supported this with movements to improve flexibility and ankle function.

Improving Range of Motion – Home Exercises
Home exercises included stretches for the calf and soleus muscles, self-mobilizations for joint flexibility, and passive ankle movements. These exercises encouraged greater range of motion while protecting healing tissues.

Maximizing Strengthening
Strength training targeted the climber’s ankle and foot, progressively rebuilding the muscle power needed for climbing. This phase emphasized controlled movements to regain the stability and strength required for weight-bearing activities.

Optimizing Stability
Dynamic stability exercises, including balance work on varied surfaces, challenged the climber’s proprioception and control, essential for safe climbing. Training on uneven surfaces and directional challenges reinforced these abilities.

Return-to-Sport: Step-Up Progression
To prepare the climber for full activity, a step-up and down progression was introduced, along with drills on uneven surfaces. Neurocognitive challenges helped recondition his movement patterns, building confidence for real-world scenarios.

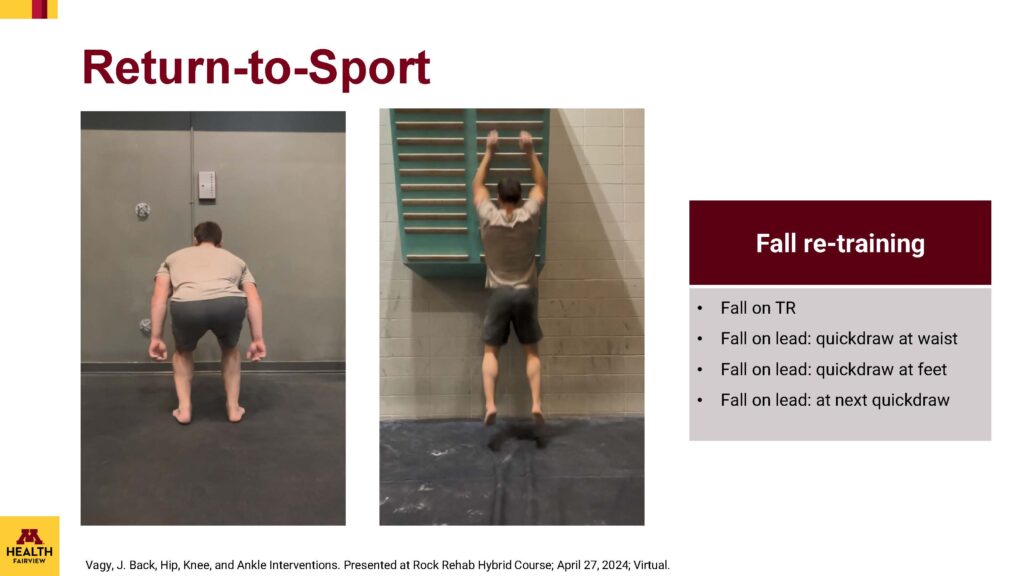
Return-to-Sport: Fall Retraining
Fall retraining introduced gradual exposure to climbing falls, from top-rope to lead climbing falls. This training, crucial for a climber, helped the patient rebuild mental resilience and trust in his physical recovery.
Outcome
At six weeks post-program, the climber returned to indoor top-rope climbing without pain. By 12 weeks, he progressed to lead climbing outdoors and resumed activities like kite surfing, salsa dancing, and slacklining, although some soreness persisted with extended walking.

About the Author
Dr. Allison Tran, a physical therapist and a board-certified orthopedic clinical specialist. You can find her at @allitran_dpt
- Disclaimer – The content here is designed for information & education purposes only and the content is not intended for medical advice.

Related Posts