Therapeutic Climbing: A Pediatric Top-Rope Rock Climbing Program for Sensory Integration Through Social Prescribing

Introduction to Sensory Integration
Sensory Integration (SI) is a theory and model developed by Jane Aryes in 1972. It gives name to neurological processes that determine how the brain organizes, interprets, and deciphers what to do with incoming sensory information- from both outside ourselves in the world around us, as well as from inside our bodies (interoception) (Ayres, 2005). Providing children with SI in the form of rich multisensory experiences has been shown to heavily improve the physical, cognitive, and social-emotional development of children with sensory processing dysfunction. Physical exercise has also been shown to have benefits for children with sensory impairments (Castano et. al., 2024). This article discusses the foreseen benefits that top-rope rock climbing can have on the overall health, wellness, and development of children by way of using SI and Sensory Processing (SP) through skilled occupational therapy (OT) interventions and leisure activities, through the model of social prescribing.
Target Population
There are many different forms of sensory dysfunction, dysregulation, and disorders. Some come foundationally from sensory processing disorders (i.e Sensory Processing Disorder (SPD), Autism Spectrum Disorder (ASD), Developmental Coordination Disorder (DCD), and Attention Hyper-Deficit Disorder (ADHD) (Van Hecke et. al., 2019). However, some sensory processing impairments such as vestibular irregularities are rooted in other ailments or disorders such as vestibular migraines, benign paroxysmal vertigo of childhood (BPVC), and central nervous system disorders (Rine et. al., 2013). These disorders may cause dizziness, vertigo, gravitational insecurity, associated anxiety/panic, and overall hypersensitivity of the vestibular and visual systems. While these children’s symptoms and deficits don’t primarily originate from that of a sensory processing diagnosis, these children could also benefit from SI as well. This is due to the knowledge that strengthening and incorporating other sensory systems, as seen in practice, will help to regulate the body and mind in those with chronic vestibular hypersensitivity.
Common Sensory Processing Related Deficits
There are many forms of dysfunction that come in part when a child has vestibular or other sensory impairments. Most commonly, these deficits impact their everyday lives. While it is not an exhaustive list, many children with these sensory difficulties have trouble with: balance, coordination, postural control, gravitational insecurity, endurance, strength, and other motor and visual skills. In addition, these children also experience emotional, cognitive, and social deficits such as: anxiety, depression, emotional dysregulation, lower-level academics, low social engagement, and social exclusion (Van Hecke et. al., 2019).
Supporting Evidence
Evidence for SI and SP
SI and SP demonstrate how engaging the senses in a way that is tailored to the child, can have many positive benefits and improve the child’s response to sensations, thus helping them be better regulated and able to perform appropriately in their other occupations in life (i.e academics, play, social participation, self-regulation, motor skills, communication skills, self-care, etc) (Camarata et. al., 2020).
Evidence for Physical Activity
There is also evidence showing support that physical exercise is beneficial to kids with sensory difficulties and with disorders such as SPD, ASD, ADHD, etc. (Ge et. al., 2025). Through meaningful exercise, there have been improvements seen in vestibular function and balance (Fong et. al., 2012) as well as postural control, praxis, strength, coordination, motor skills, cognition, speed, emotional regulation, and social skills (Aykora et. al., 2019).
Therapeutic Benefits of Rock Climbing

Climbing and Proprioception
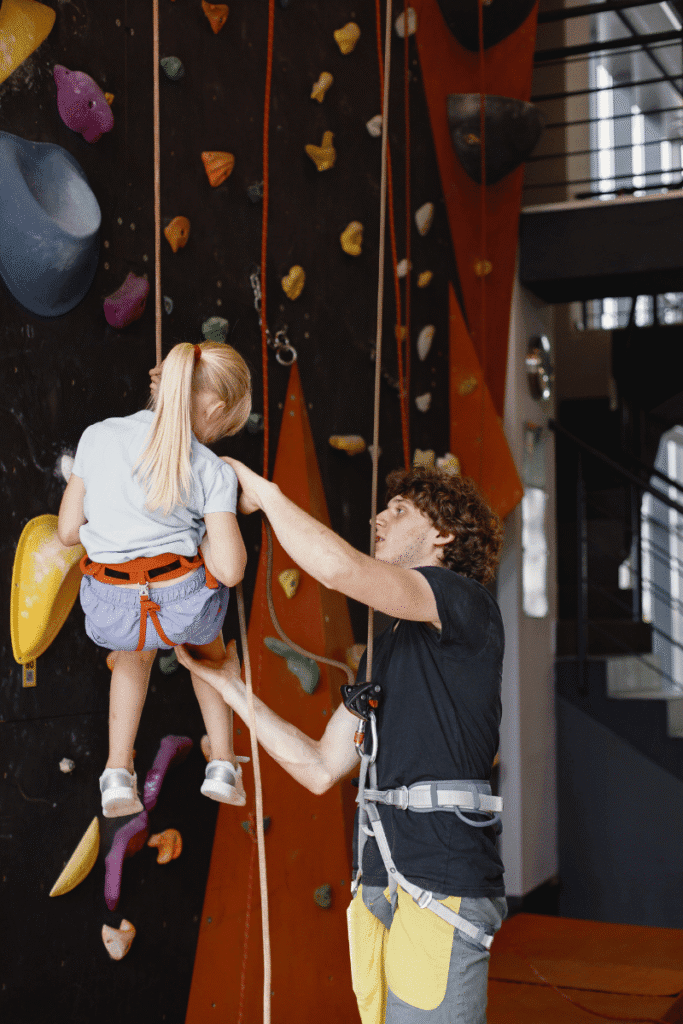
Incorporating climbing into the lives of these children provides them opportunities to combine SI with exercise as a purposeful OT intervention and/or leisure activity. Climbing heavily involves proprioception as the climber has to continually receive and interpret proprioceptive input from the rocks/holds, their hands, feet, and the harness, as they shift their body weight to target the rocks/holds they need to climb to and use their strength to lift, pull, and push their way up the wall through a variety of both static and dynamic, weight-bearing movements (Klymus et. al., 2023).

Climbing and Tactile Input
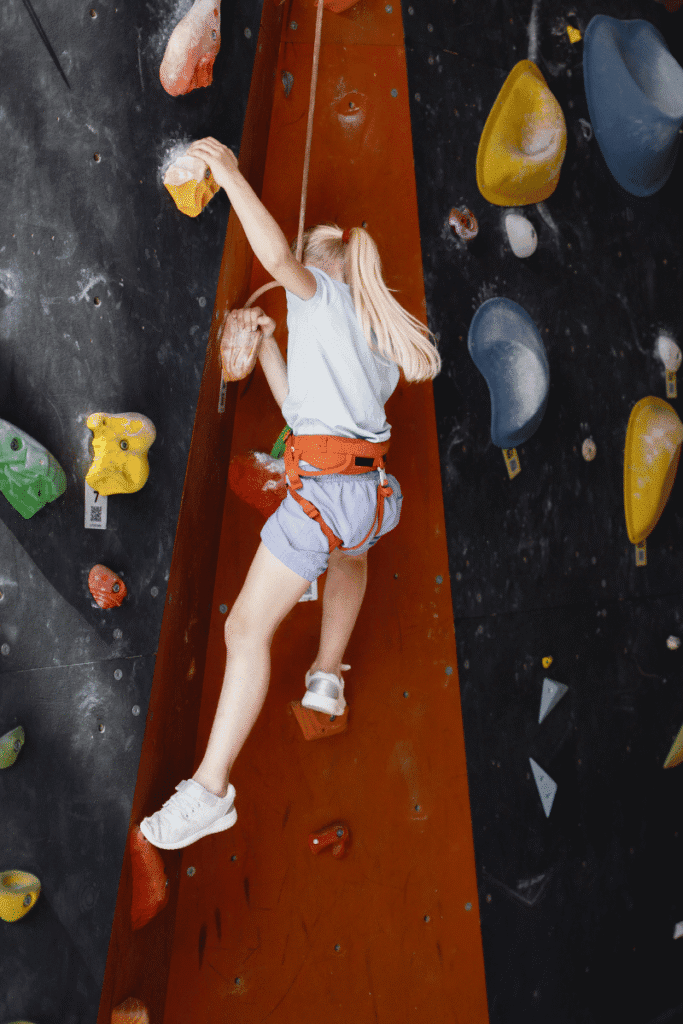
Another sensory system that is heavily involved in climbing is the tactile system. Having exposure to different tactile sensations has been shown to improve tactile processing and decrease a child’s tactile defensiveness (Camarata et. al., 2020). Climbing provides a rich tactile experience as there are many different holds with varying sizes, shapes, and textures. The climber also may choose to use chalk throughout their climb as wanted/needed to improve their ability to execute an initial grasp as well as maintain their grip once they have made contact with a hold.

Climbing and and Motor Coordination
Climbing also requires motor coordination and praxis. Climbers use their whole body to move up the wall, requiring motor planning, eye-hand coordination, balance, muscle strength, postural control, reaction time, reaching, as well as other gross & fine motor skills (Liu et. al., 2022). Children that have sensory impairments often need help with some if not all of these skills (Klymus et. al., 2023). Climbing also helps children develop better fine motor skills such as grip and finger strength, both of which can translate over to better participation in I/ADL tasks through generalization.
Emotional and Social Aspects of Sensory Integration
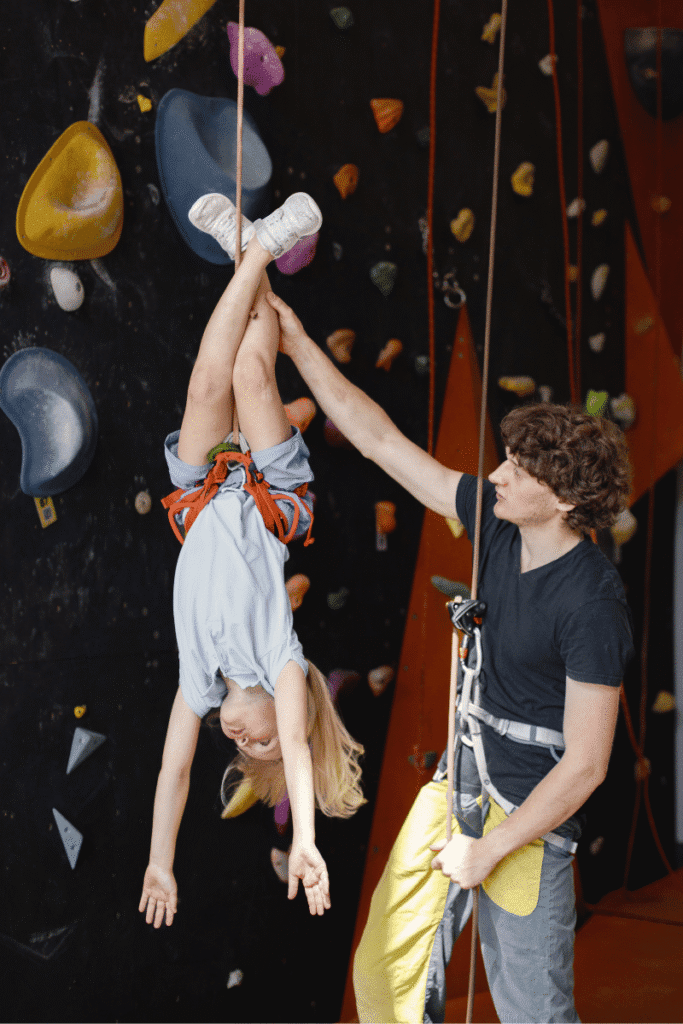
Climbing can also help improve a child’s mental health, social interactions, self-confidence, and self-efficacy. (Mazzoni, 2009). Climbing gives the child a sense of mastery and intrinsic motivation that comes from problem solving as they go up the wall (Ceciliani et. al., 2008). Incorporating top rope climbing specifically has great potential to help children socially as it requires being tied to their belayer (climbing partner) on the ground. This would provide them the opportunity to practice trust and communication skills (Liu et. al., 2022). Top-rope climbing (TRC) also has the potential to help children lower their levels of anxiety and depression as the child is moving their body, balancing their sensory systems, and achieving a sense of self-accomplishment and mastery. Many children with vestibular deficits/difficulties most likely will have anxiety (Bart et. al., 2009) as they may be dealing with or are afraid of provoking gravitational insecurity, feelings of dizziness, vertigo, etc that can evoke a lot of fear. Therefore, kids with vestibular issues especially may have fear when it comes to rock climbing (May-Benson et. al., 2020). However, through using proprioception and repeated exposure to the linear-and therefore more tolerable, raising and lowering of the body to the ground, in a way that the climber can control the movement, vestibular sensitivity may decrease and/or the child will have less vestibular-triggered fear.
Climbing and Autism Spectrum Disorder (ASD)
Many children with sensory processing deficits also have Autism Spectrum Disorder (ASD) Patil, O., & Kaple, M. (2023). Rock climbing can be appealing to children with autism for many reasons. Some children with autism enjoy risk-seeking behaviors such as climbing or jumping (Fahy et. al., 2020). TRC would give them a safe and appropriate environment to do so. Kids with ASD also may enjoy the simplicity of rock climbing, as there isn’t much sequencing, and there is just one main objective-to get to the top of the wall. These kids also may enjoy the fact that each climb ends with completion of a task, which is a big draw for a lot of children with ASD, seeing a task through from start to finish. Expectations are also clear, with routes outlined for them by color so all they have to do is follow the correct color up the wall, which also outlines a more straightforward pathway to completion/the goal, which may not be as clear in other sports. Kids also may enjoy that rock climbing can be performed at varying levels concurrently with others (should they choose to climb with a group) and that their performance on the wall doesn’t include physical contact with other people, there aren’t social cues to navigate, and they don’t or have people relying on them to score points like they do in team sports.

How Rock Climbing is Currently Being Used in Pediatric OT
Currently, in some pediatric occupational therapy clinics there are short rock walls where children can boulder (a form of climbing performed without being secured by a harness and rope for safety). While this is beneficial to an extent, there is reason to believe that the use of a harness and rope as used during TRC would benefit kids more than that of bouldering.
For example, if a child is bouldering, they know they aren’t fully secure, leading to fear, especially for a child with hypersensitive systems, which can lead to lack of motivation to try the wall, or get as much out of the wall (i.e working on various sensory, motor, and other goals) as they don’t feel as free to move due to the fear of falling. The harness provides more feelings of safety and security which would allow the child to more fully participate in climbing.
Sensory Integration theory says that tactile, visual, and vestibular are three sensory systems that work very close together. TRC allows for sensory-rich exposure in these areas. Proprioception helps to decrease sensory overload from the vestibular system. Therefore, it is also hypothesized that the extra proprioceptive input from the harness at the hips will allow for better sensory integration of the child, being that the more proprioceptive feedback there is, the more balanced the child’s vestibular system (for example) will feel.

The Therapist’s Perspective
In addition, some occupational therapists currently might not feel totally comfortable facilitating a child up the rock wall in its current state because a child could fall on them if they don’t feel strong enough to hold the child. The child can also only get as far off of the ground as the therapist can reach, which isn’t far at all. The therapist may also be hesitant to use the rock wall in its current bouldering state because there is more danger due to the falling typically necessary in order to get down from the wall. Although crash pads are in place under the child, the child does still have to land on the ground abruptly, with various points that they could make contact, which isn’t as safe as compared to top-rope climbing where the child would be slowly lowered down to the ground, feet first.
Therapeutic Climbing Through the Social Prescribing Model
Social prescribing is a newer model that is currently being used primarily in the U.K. Through this model, patients can be connected to resources outside of clinical care in their community to receive additional wellness support through social connectedness and meaningful activities (World Health Organization, 2021). Patients are connected with a link worker who assesses the needs and goals of the patient, and works with them to fill in any gaps in care with activities and/or programs for group learning, physical exercise, and community/social engagement, for example (Bradley & Scott, 2021). After identifying the goals of the patient, the link person helps them create an action plan to address their goals and connects them with the appropriate resources. A rock climbing program for kids with sensory disorders and dysfunction, overseen by occupational therapists and trained climbing coaches, in addition to OT sessions would be beneficial for these children’s physical and emotional health as well as improve social skills. The idea is that improvement in these core areas will lead to improvements in I/ADLs and the skills that they learn, through generalization, can transfer over to other tasks and increase overall feelings of self-mastery and well-being in their daily lives.

Summary and Considerations
In summary, both SI and physical exercise have been found to be beneficial to children with sensory impairments in a variety of ways. Climbing has been found to be a therapeutic modality that can help children increase their physical, mental, and social well-being. Currently, climbing is used on a small scale for children with sensory impairments. However, there is great potential for climbing programs to be implemented and made available to those children with sensory difficulties, allowing them to work on a number of skills that will help them in their daily occupations in life such as academics, play, social, self-care, and participation (Kompán et. al., 2021). Social Prescribing is a means by which these children could become aware of and receive access to these climbing programs.
Social Prescribing Process for Children and Youth
Discussion with client and family regarding the purpose of social prescribing.
Sample: Social prescribing is a focused method to link clients receiving healthcare services, such as occupational therapy, to community activities to promote health and well-being. This helps clients increase community access, social participation, and leisure participation all while supporting their therapy goals.
Evaluation
Evaluate client’s preferences and participation patterns using the Children’s Preferences for Participation and Enjoyment (CAPE) and the Preferences for Activities for Children (PAC) to determine the client’s interests and identify activities they are not currently participating in but would like to, especially those that could support their occupational therapy goals. Couple this with their occupational therapy assessment results to identify strengths in sensory and motor skills to help determine the best community-based activity.
Contact the Community Site
See the Social Prescribing Tool Kit on how to form relationships with community sites.
Connect Client and Community Site Using Link Worker
Facilitate the communication between the link worker and the site. Ensure clients and the site administrator have completed the provided intake questionnaires. The link worker should ensure that the intake questionnaires are completed and information is shared with the community site.
Communication and Progress Monitoring
Establish a method of communication between community site and occupational therapist. Provide method of progress monitoring and consistent communication using the link worker.
Implementation
Implement the social prescribing with concurrent occupational therapy services.
Social Prescribing Toolkit Template (for OTs)
A Social Prescribing Toolkit was designed to support OTs in effectively implementing social prescribing programs and interventions. It provides a structured approach to identifying, referring, and monitoring clients as they engage with community-based support. Top rope rock climbing (TRC) was used as an example for how the Social Prescribing Toolkit can be used. Please reach out to Julianne for more detailed information about the specifics of the program.
- Describes how (TRC) can be beneficial as a modality for social prescribing
- Identifies the implementation team and their roles
- Plan, Do, Study, Act as the framework
- Describes how (TRC) is a good option for patients from an occupational therapy standpoint (i.e what skills it helps kids work on)
- Operational management
- Target population
- Value
- Anticipated needs
- Program objectives
- Roles of the team
- Funding
- Referral pathway
- How link workers get connected to patients
- How to Monitor and Evaluate program participants
- Activities/Interventions
- Preparatory interventions
- Interventions/activities while in the program
Identifies any similar or relevant programs in the community, if any.
- Describes link worker training and process
- Evaluation:
- Children’s Assessment of Participation and Enjoyment (CAPE)
- Preferences of Activities for Children (PAC)
- OT Likert Scale Questions
- Coach Likert Scale Questions
- Pre and Post Assessment forms for the patient and their families
- Pre and Post Assessment forms for OTs
- Goal Attainment Scale (GAS)
- Coach Communication Log
- Family Communication Log
- Handout-Sensory Processing, Sensory Integration and the Benefits of Rock Climbing
- Rock climbing program flyer for interested patients and their families, referral sources

Author Bio
Julianne Kindt is an occupational therapist practicing in Arizona. She graduated with her Doctorate of Occupational Therapy from Northern Arizona University and received her Bachelor of Science degree from Brigham Young University. She first started climbing in college and has loved it ever since! Early on in school she realized that she wanted to combine her passion for rock climbing, occupational therapy, and interest in working with people with neurological disorders. This led her to develop a rock climbing program for sensory integration as well as motor, cognitive, and social-emotional skill development. She will be presenting this program at the annual American Occupational Therapy Association (AOTA) conference in April 2026.
To connect or discuss additional details about the program please email: juliannekindt@gmail.com
References
- Almovist, L., Granlund, M., Krumlinde-Sundholm, L., Ullenhag, A. (2012). Cultural validity of the Children’s Assessment of Participation and Enjoyment/Preferences for Activities of Children (CAPE/PAC). Scandinavian Journal of Occupational Therapy, 19, 428–438. DOI: 10.3109/11038128.2011.631218
- Anastasiadi, I., Tzetzis, G. (2013). Construct validation of the greek version of the Children’s Assessment of Participation and Enjoyment (CAPE) and Preferences for Activities of Children (PAC). Journal of Physical Activity & Health,10.4, 523-532. Retrieved from https://eds.a.ebscohost.com.p.atsu.edu/eds/pdfviewer/pdfviewer?sid=ff14a6f0-b827-464e-b81c-29dcb270afca%40sessionmgr4002&vid=7&hid=4203
- Aykora, E. (2019). An analysis over physical and physiological parameters of elementary school children taking part in a sport climbing exercise. Universal Journal of Educational Research, 7(2), 624–628.
- Ayres, A. J. (2005). Sensory integration and the child. Western Psychological Services.
- Bart, O., Bar-Haim, Y., Weizman, E., Levin, M., Sadeh, A., & Mintz, M. (2009). Balance treatment ameliorates anxiety and increases self-esteem in children with comorbid anxiety and balance disorder. Research in Developmental Disabilities, 30(3), 486–495. https://doi.org/10.1016/j.ridd.2008.07.008
- Bradley, G., & Scott, J. (2023). Social prescribing nomenclature, occupational therapy and the theory of institutional work: Creating, maintaining and disrupting medical dominance. Occupational Therapy in Health Care, 37(1), 40–53. https://doi.org/10.1080/07380577.2021.1926046
- Camarata, S., Miller, L. J., & Wallace, M. T. (2020). Evaluating sensory integration/sensory processing treatment: Issues and analysis. Frontiers in Integrative Neuroscience, 14, Article 556660. https://doi.org/10.3389/fnint.2020.556660
- Castaño, P. R. L., Suárez, D. P. M., González, E. R., Robledo-Castro, C., Hederich-Martínez, C., Cadena, H. P. G., Vargas, P. A. S., & Montenegro, L. C. G. (2024). Effects of physical exercise on gross motor skills in children with autism spectrum disorder. Journal of Autism and Developmental Disorders, 54(8), 2816–2825. https://doi.org/10.1007/s10803-023-06031-5
- Ceciliani, A., Bardella, L., Grasso, M. L., Zabonati, A., & Robazza, C. (2008). Effects of a physical education program on children’s attitudes and emotions associated with sport climbing. Perceptual and Motor Skills, 106(3), 775–784. https://doi.org/10.2466/pms.106.3.775-784
- Fahy, S., Delicâte, N., & Lynch, H. (2020). Now, being, occupational: Outdoor play and children with autism. Journal of Occupational Science, 28(1), 114–132. https://doi.org/10.1080/14427591.2020.1816207
- Fong, S. S., Fu, S. N., & Ng, G. Y. (2012). Taekwondo training speeds up the development of balance and sensory functions in young adolescents. Journal of Science and Medicine in Sport, 15(1), 64–68. https://doi.org/10.1016/j.jsams.2011.06.001
- Ge, S., Guo, X., Jiang, B. Y., Cordova, A., Guan, J., Zhang, J. Q., & Yao, W. X. (2025). Improving sensory integration in Chinese children with moderate sensory integration challenges through engaging basketball training. Frontiers in Psychology, 15, 1481945. https://doi.org/10.3389/fpsyg.2024.1481945
- Hanna, S., Hurley, P., Kertoy, M., King, G., King, S., Law, M.,…Young, N. (2004). Children’s Assessment of Participation and enjoyment & Preferences for Activities of Children. San Antonio, TX: Pearson.
- Kaplan-Reimer, H., Sidener, T. M., Reeve, K. F., & Sidener, D. (2011). Using stimulus control procedures to teach indoor rock climbing to children with autism. Behavioral Interventions, 26(1), 29–49. https://doi.org/10.1002/bin.315
- Klymus, T. M., Ravchyna, T. V., Herus, O., Kozak, M. Y., Tiurina, T. G., Shkoliar, M. V., & Marcucci, G. (2023). Using the sensory integration technique for people with autism spectrum disorders during training at the climbing section. Polski Merkuriusz Lekarski, 558, 33–37.
- Kompán, J., Svidroňová, M. M., & Maslen, M. (2021). Climbing literacy project for children and youth: A utility analysis. Journal of Physical Education and Sport, 21, 2074–2080. https://doi.org/10.7752/jpes.2021.s3264
- Liu, S., Gong, X., Li, H., & Li, Y. (2022). The origin, application and mechanism of therapeutic climbing: A narrative review. International Journal of Environmental Research and Public Health, 19(15), 9696. https://doi.org/10.3390/ijerph19159696
- May-Benson, T. A., Lopes de Mello Gentil, J., & Teasdale, A. (2020). Characteristics and prevalence of gravitational insecurity in children with sensory processing dysfunction. Research in Developmental Disabilities, 101, 103640. https://doi.org/10.1016/j.ridd.2020.103640
- Mazzoni, E. R., Purves, P. L., Southward, J., Rhodes, R. E., & Temple, V. A. (2009). Effect of indoor wall climbing on self-efficacy and self-perceptions of children with special needs. Adapted Physical Activity Quarterly, 26(3), 259–273. https://doi.org/10.1123/apaq.26.3.259
- Patil, O., & Kaple, M. (2023). Sensory processing differences in individuals with autism spectrum disorder: A narrative review of underlying mechanisms and sensory-based interventions. Cureus, 15(10), e48020. https://doi.org/10.7759/cureus.48020
- Rine, R. M., & Wiener-Vacher, S. (2013). Evaluation and treatment of vestibular dysfunction in children. NeuroRehabilitation, 32(3), 507–518. https://doi.org/10.3233/NRE-130873
- Van Hecke, R., Danneels, M., Dhooge, I., Van Waelvelde, H., Wiersema, J. R., Deconinck, F. J. A., & Maes, L. (2019). Vestibular function in children with neurodevelopmental disorders: A systematic review. Journal of Autism and Developmental Disorders, 49(8), 3328–3350. https://doi.org/10.1007/s10803-019-04059-0
- World Health Organization. (2021). World report on hearing. https://www.who.int/publications/i/item/9789290619765
- Disclaimer – The content here is designed for information & education purposes only and the content is not intended for medical advice.

Related Posts