Scapholunate Ligament Injury – Case Study and Return to Climbing Protocol
This presentation presents a detailed case study on a scapholunate ligament injury, providing a comprehensive look at the anatomy, biomechanics, injury history, rehabilitation protocol, and the climber’s return to sport. Led by Rachel Rubin-Sarganis and Waldo Cheung, both highly qualified physical therapists with advanced degrees, this session explores the unique challenges of treating climbing-specific injuries, with insights into effective interventions and progress tracking.
Topics Covered:
- Anatomy and biomechanics of the scaphoid – Injury mechanism and assessment
- Step-by-step rehabilitation phases tailored for climbers
- Load management for safe progression in climbing
Learning Objectives:
- Understand scapholunate ligament injury mechanisms, diagnostics, and treatment
- Gain insights into the demands of climbing-specific loads on the wrist
- Learn about progressive, sport-specific rehabilitation to aid climbers in their journey back to the sport
Introduction
This case study focuses on scapholunate ligament (SLL) injury management in a climber. It includes an anatomical overview, injury specifics, rehabilitation protocol, and the climber’s return to sport. The study also examines current challenges and limitations in scapholunate ligament rehabilitation.

Anatomic Overview of the Scaphoid
The scaphoid is a small, boat-shaped bone in the wrist that plays a key role in load transmission from the hand to the forearm. It has a high risk of injury, especially in falls. Its blood supply is primarily retrograde, making it vulnerable to conditions like avascular necrosis.
Axial Loading and Scaphoid Stability
The scapholunate and radioscaphocapitate ligaments are primary stabilizers of the scaphoid. Secondary and dynamic stabilizers further contribute to scaphoid stability, involving various wrist and forearm muscles essential for function and injury prevention.
Climbing-Specific Loads on the Scaphoid
Climbing exerts specific, intense forces on the scaphoid. Movements like compression, underclings, gastons, and mantling place high loads on the scaphoid, while dynamic moves introduce sudden and unpredictable stress, increasing injury risk.
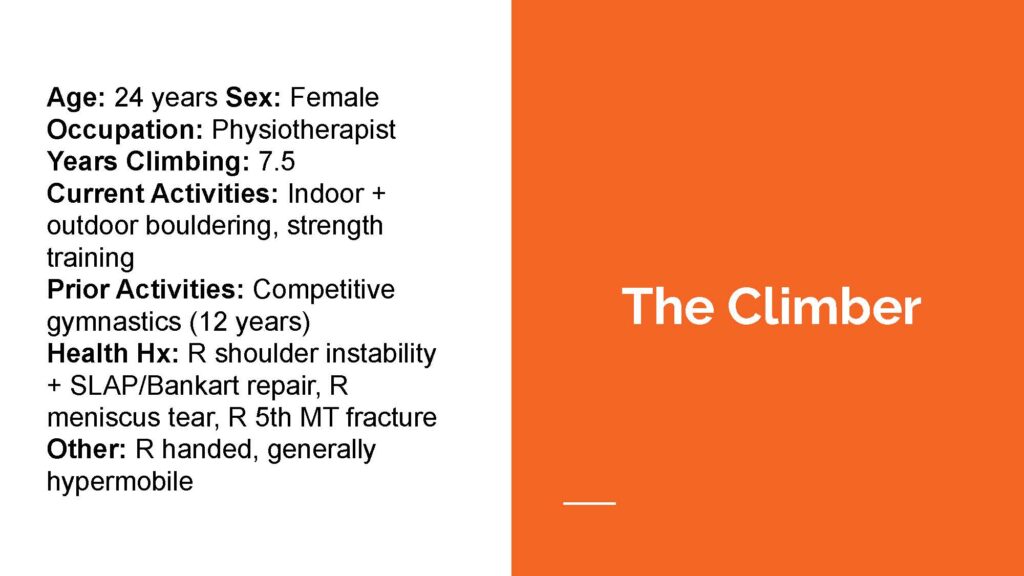
The Climber’s Profile
The climber, a 24-year-old physiotherapist with seven years of climbing experience, has a history in competitive gymnastics and pre-existing injuries, including shoulder instability and meniscus tears. This background and her hypermobility may affect her injury recovery and rehabilitation strategy.
Injury History
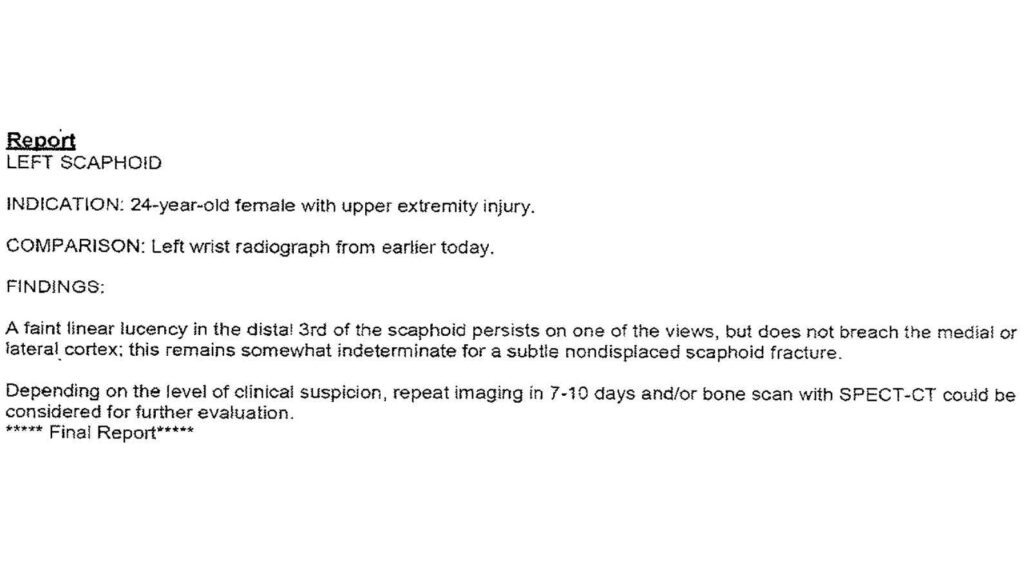
The climber’s injury occurred when she slipped on ice, resulting in a FOOSH (fall on outstretched hand) with hyperextension of the wrist. Initial X-rays were inconclusive, and after immobilization, further imaging did not reveal a fracture, although symptoms persisted.
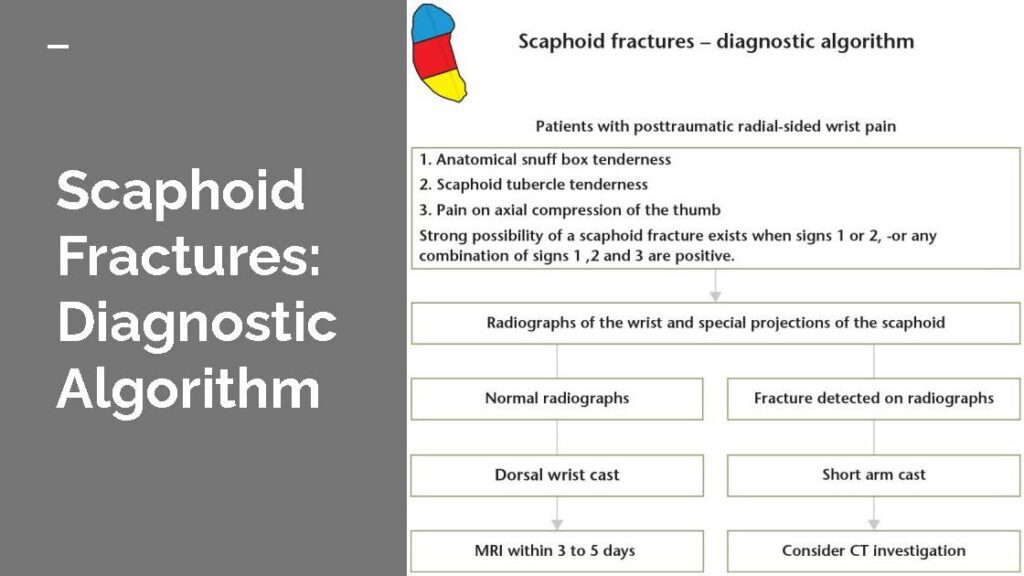
Diagnostic Tests for Scaphoid Fracture
Key clinical tests to assess scaphoid injuries include the scaphoid tubercle tenderness, anatomical snuff box tenderness, and axial compression. These tests offer varying levels of sensitivity and specificity for diagnosing scaphoid fractures.
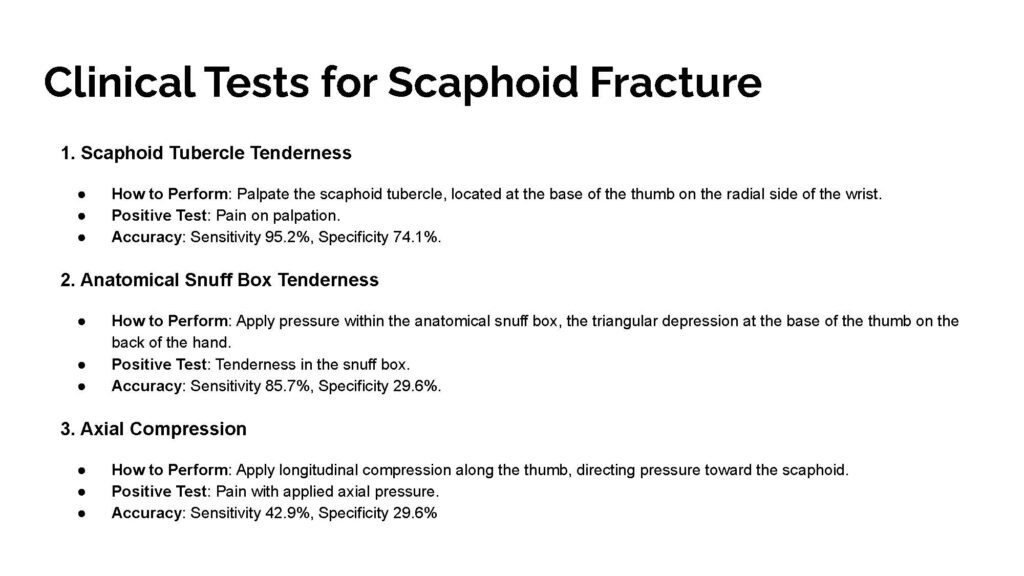
Clinical Tests for Scaphoid Fracture
Below are several clinical tests for scaphoid fractures.
Subjective Reports
The climber reported swelling, pain on the radial side of the wrist, and sensitivity to activities like weight-bearing and gripping. While immobilization helped, it also led to nerve symptoms, emphasizing the complexity of treating wrist injuries in climbers.
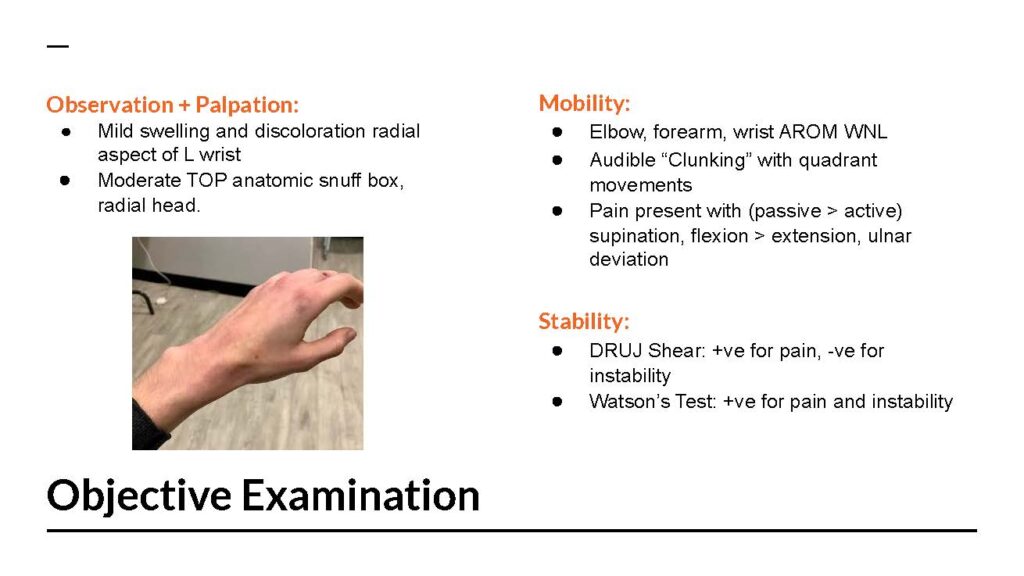
Objective Examination
An examination revealed swelling, tenderness, reduced range of motion, and instability. Specific tests, such as the Watson’s Test, confirmed pain and instability in the scapholunate ligament, which informed the subsequent rehabilitation plan.
Rehabilitation Protocol
The rehabilitation protocol spans several phases, from maximum protection to maintenance. It outlines detailed exercises, climbing restrictions, progression criteria, and goals for each phase, focusing on controlled recovery and safe return to sport. 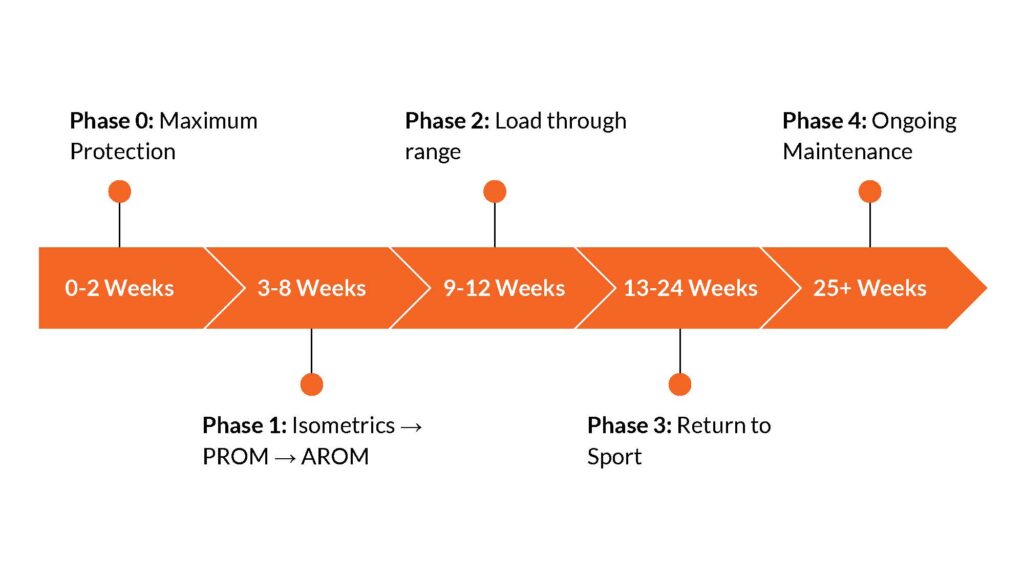
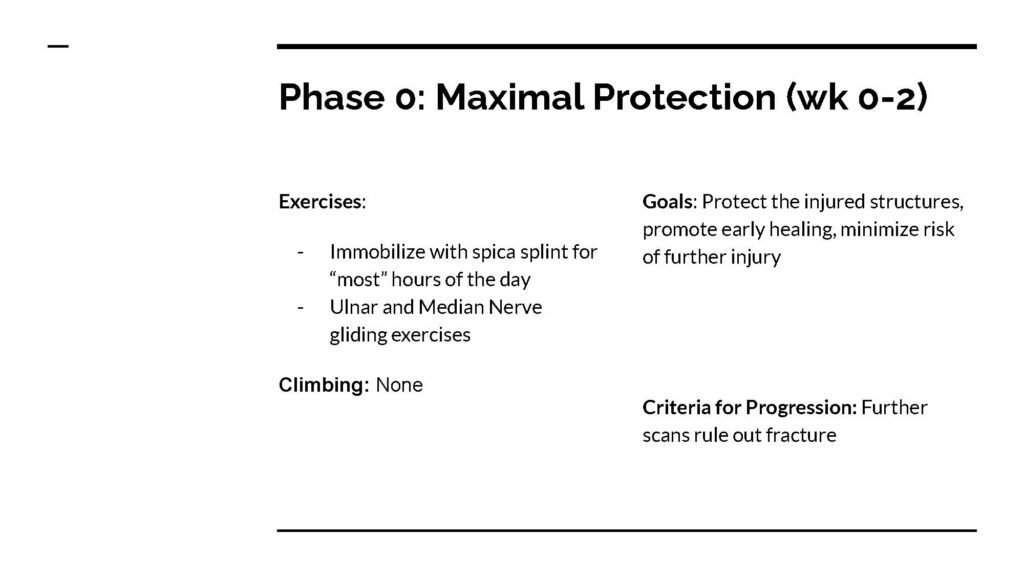
Phase 0: Maximum Protection (Weeks 0-2)
During the initial phase, the wrist is immobilized in a spica splint, with exercises limited to nerve gliding. This phase aims to protect injured structures, minimize further injury, and ensure a foundation for healing before advancing.
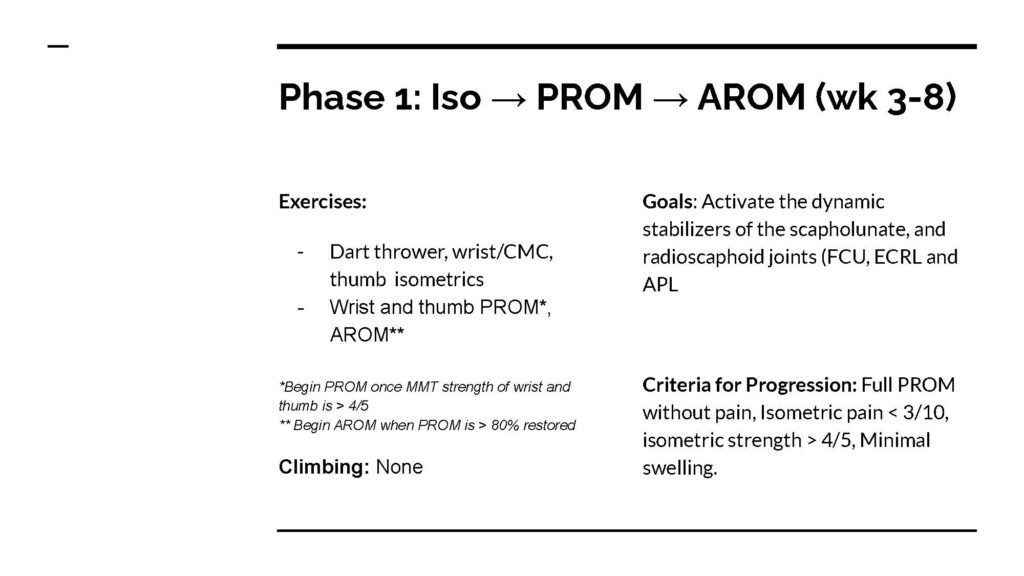
Phase 1: Isometrics to AROM (Weeks 3-8)
In this phase, the climber progresses from isometric to active range of motion (AROM) exercises, focusing on activating dynamic stabilizers. Criteria for advancement include achieving specific strength and range of motion without pain.
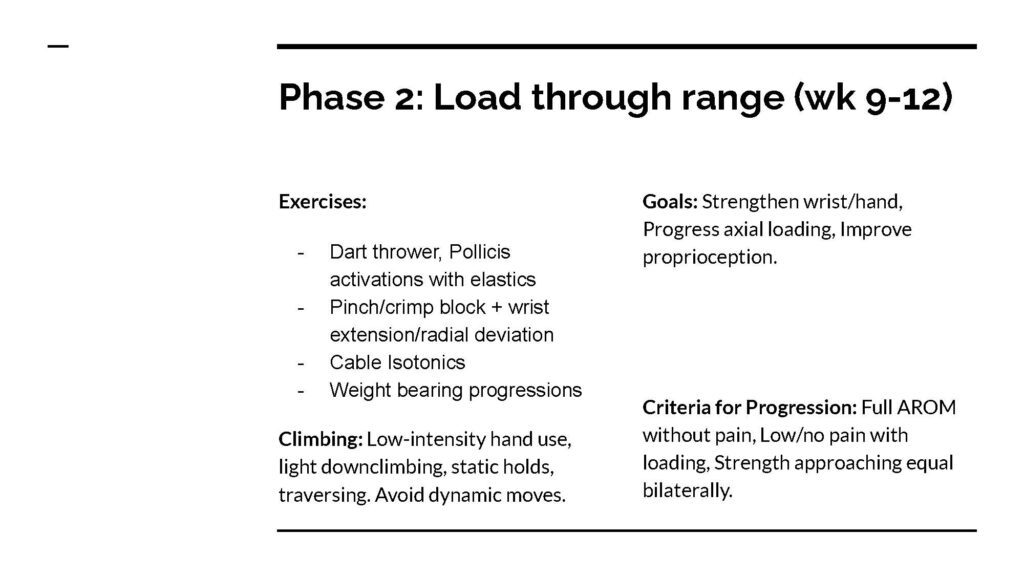
Phase 2: Load Through Range (Weeks 9-12)
This phase emphasizes loading the wrist through its range, incorporating exercises like the dart thrower’s motion and pinch block. Climbing activities are restricted to low-intensity moves to gradually rebuild strength and proprioception.
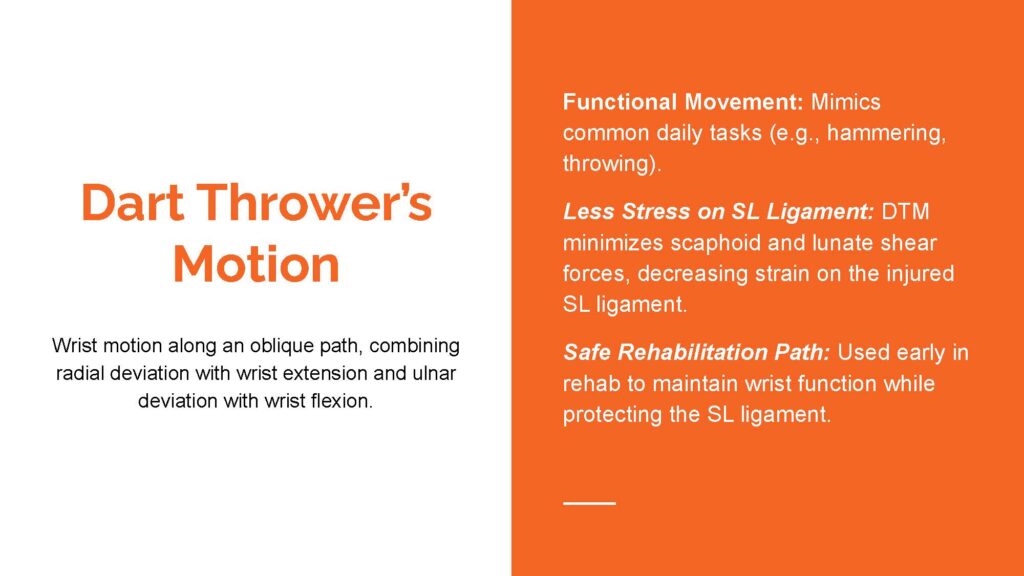
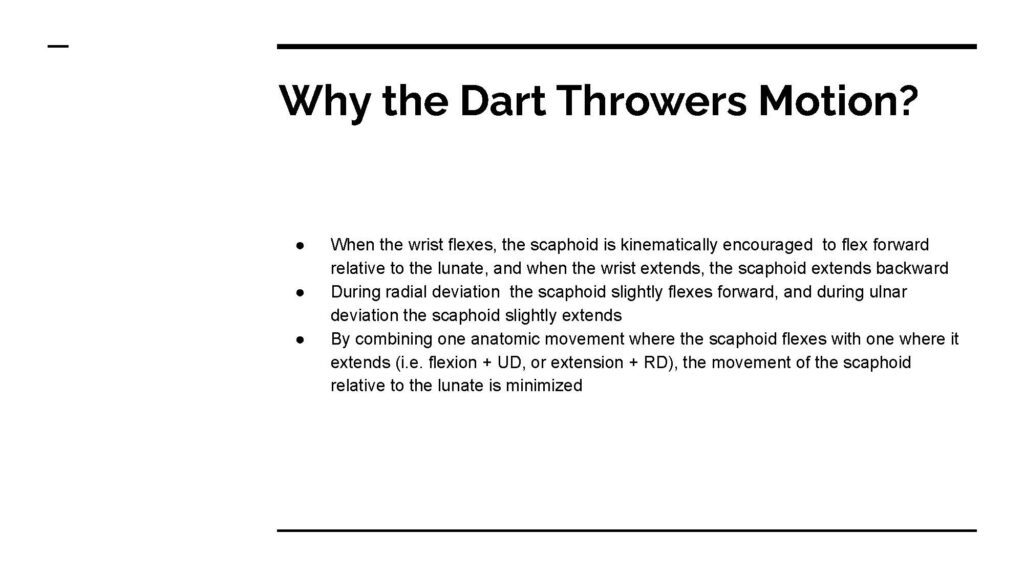
Dart Thrower’s Motion
The dart thrower’s motion is a safe wrist movement combining radial deviation with extension and ulnar deviation with flexion, minimizing strain on the scapholunate ligament. This functional motion is used early in rehab to maintain wrist mobility while protecting the injured ligament.
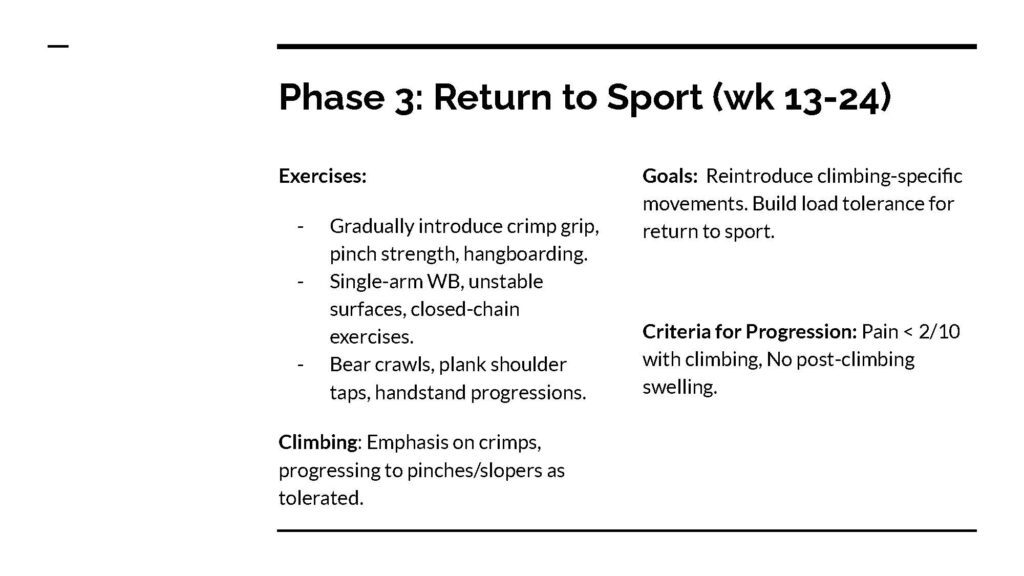
Phase 3: Return to Sport (Weeks 13-24)
With careful progression, the climber reintroduces climbing-specific movements, focusing on strengthening grips and managing load tolerance. The goal is to safely reintroduce full climbing activity without triggering pain or swelling.
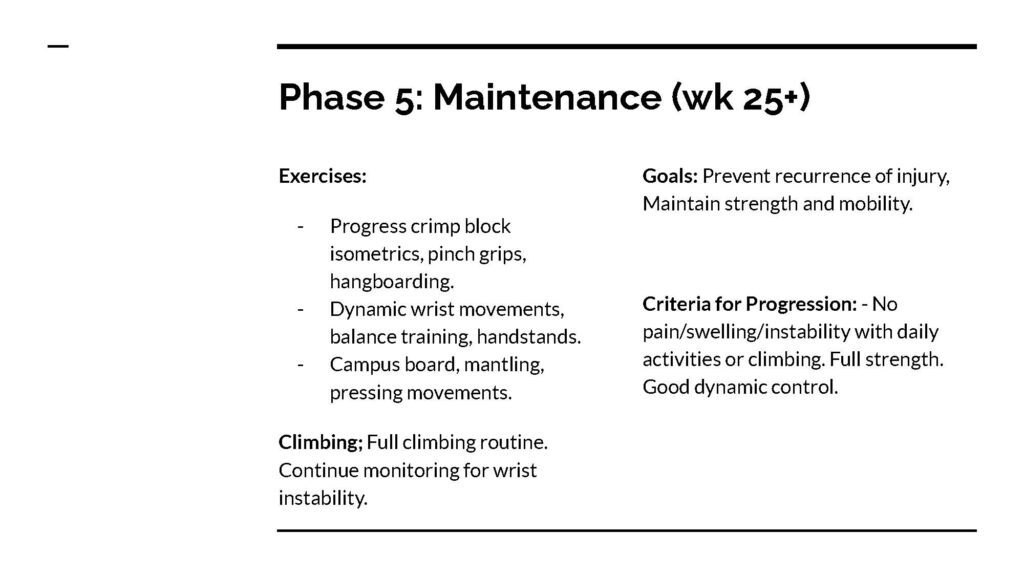
Phase 5: Maintenance (Weeks 25+)
In this phase, exercises focus on long-term strength and mobility to prevent reinjury. The climber continues a full climbing routine while monitoring for wrist instability and signs of overuse.
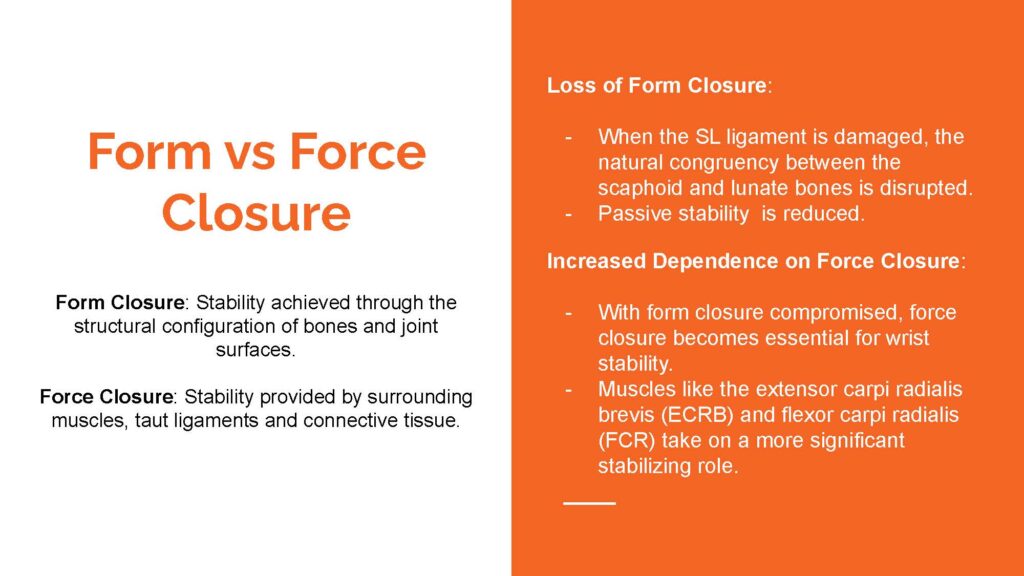
Form vs. Force Closure
In the case of SLL injury, form closure (bone structure stability) is compromised, increasing reliance on force closure from muscles and ligaments. This shift requires stronger engagement from muscles like the extensor carpi radialis brevis for wrist stability.
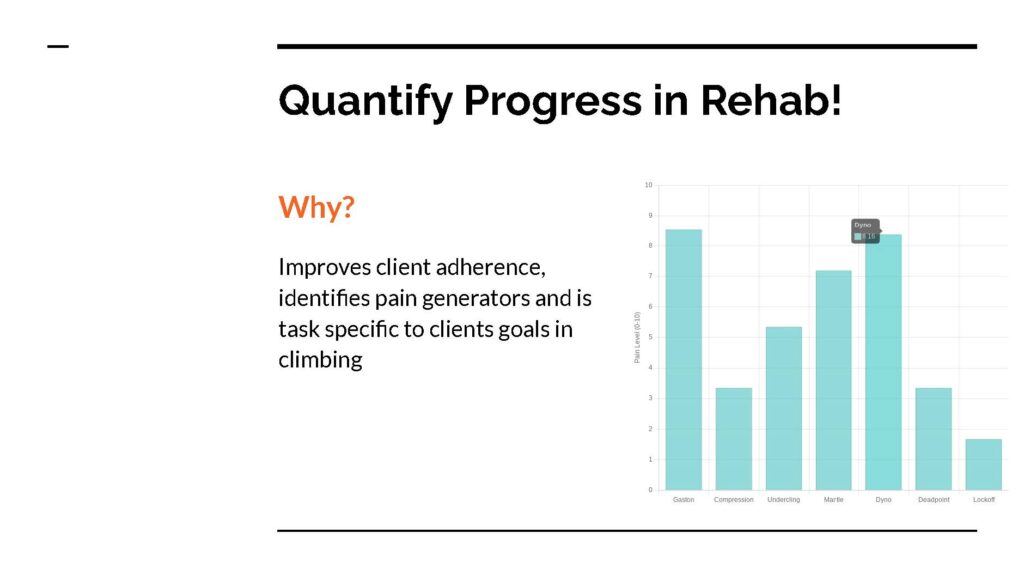
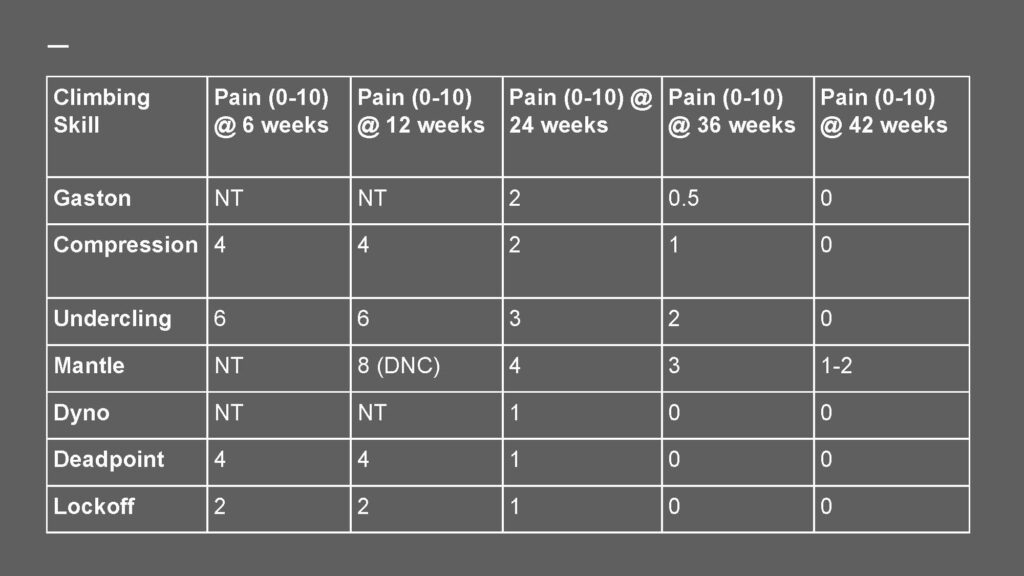
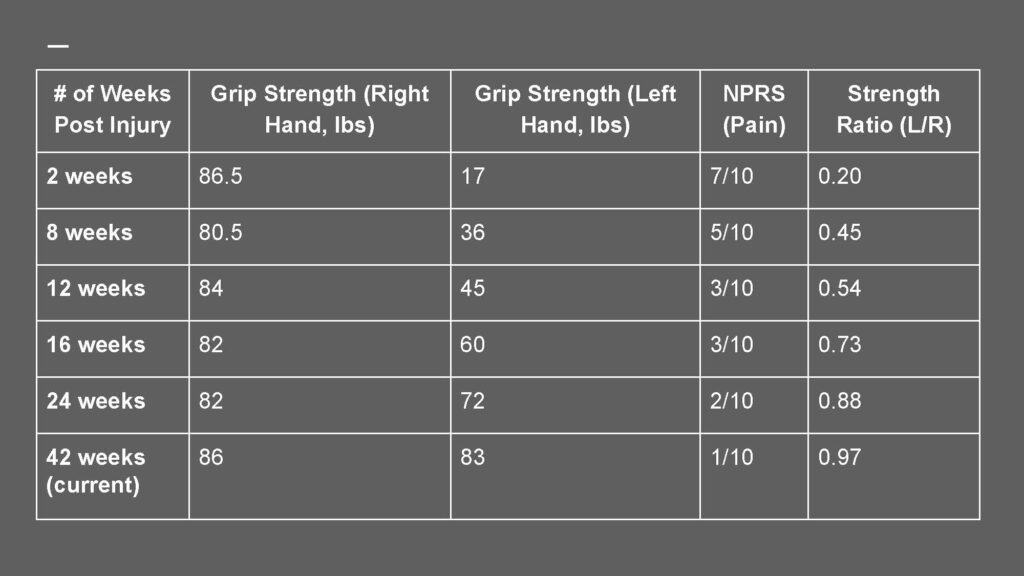
Quantifying Rehab Progress
Tracking progress enhances client adherence, helps identify pain sources, and aligns rehabilitation goals with specific climbing tasks. This approach supports measurable and client-focused recovery.
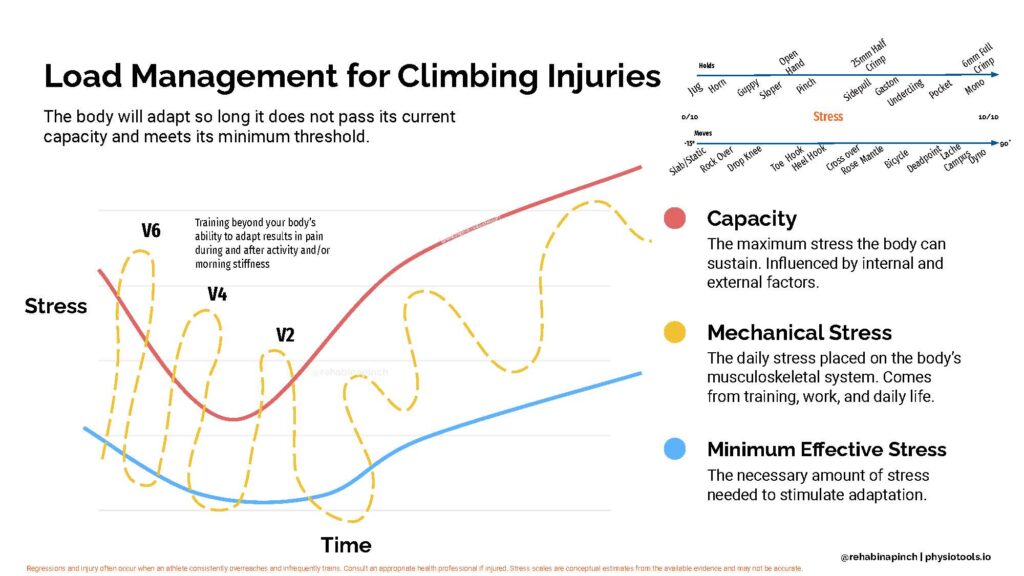
Load Management for Climbing Injuries
Effective load management is crucial for preventing injury recurrence. Rehabilitation involves balancing mechanical stress, capacity, and time to avoid exceeding the body’s current capabilities, fostering gradual adaptation.
Psychosocial Effects of Injury
Injury impacts climbers beyond physical limitations, including emotional challenges like identity loss, frustration, and isolation from their community. These factors highlight the importance of a holistic rehabilitation approach.
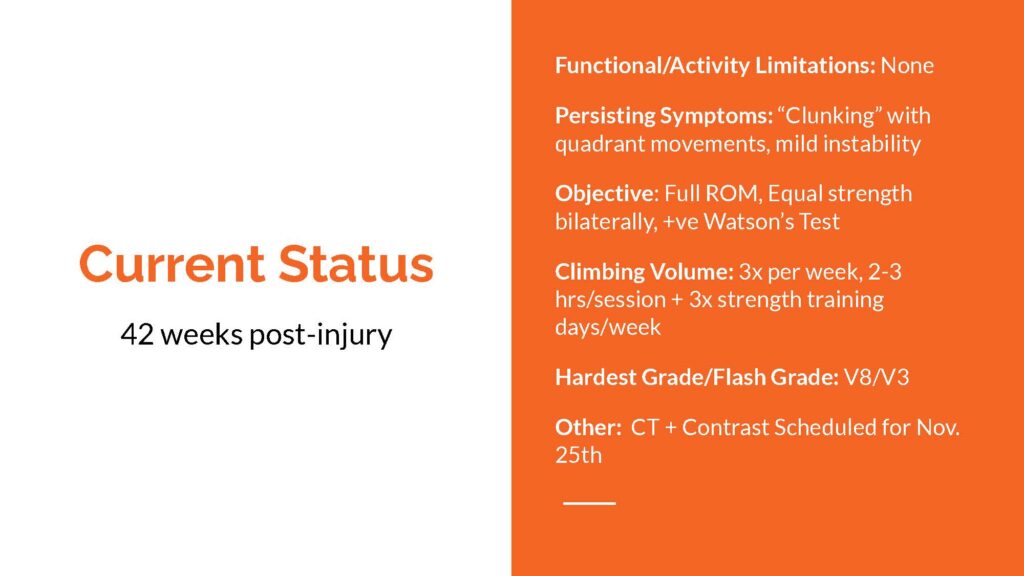
Current Patient Status
Forty-two weeks post-injury, the climber has returned to climbing three times a week. Despite occasional wrist clunking, she has regained full strength and range of motion, with minimal symptoms, marking a successful rehabilitation outcome.
Study Limitations
Limitations of this case study include its single-subject nature and potential biases, as the researcher was also the subject. Factors such as specific sports history and hypermobility may limit the generalizability of findings.
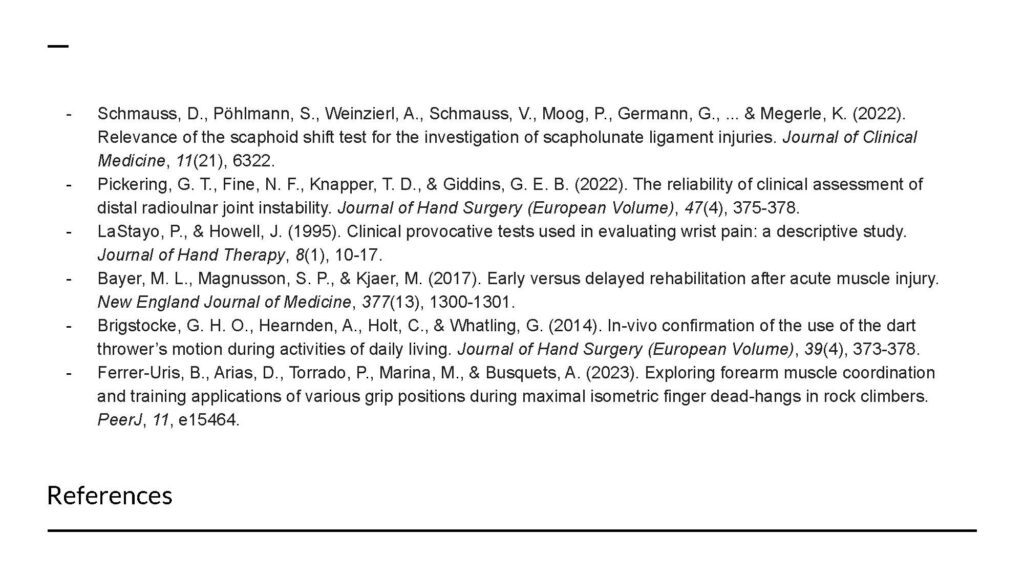
Resources
Below are the resources used in the case study
Author Bio
Rachel Rubin-Sarganis is a Physiotherapist, climbing coach, and fitness trainer at Parkway Physiotherapy in Victoria, B.C., Canada. Find her on Instagram @physio.rocks
- Disclaimer – The content here is designed for information & education purposes only and the content is not intended for medical advice.

Related Posts


